Als ein Vorreiter im Bereich des anatomischen Prothesendesigns kann LINK auf jahrzehntelange Erfahrung bei der Entwicklung dieser Schafttypen zurückgreifen. Der beeindruckende klinische Erfolg des SPII Konzepts ist im schwedischen Register umfassend dokumentiert. 2
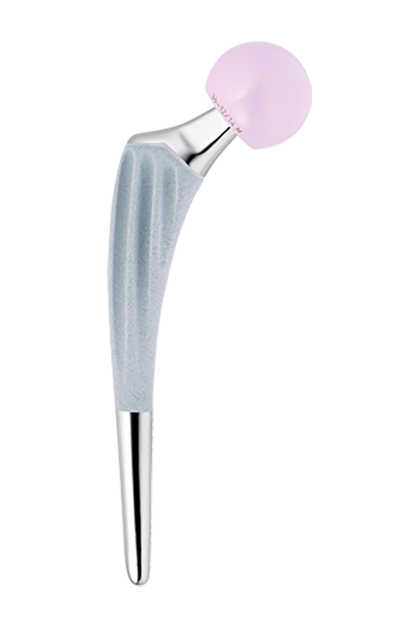
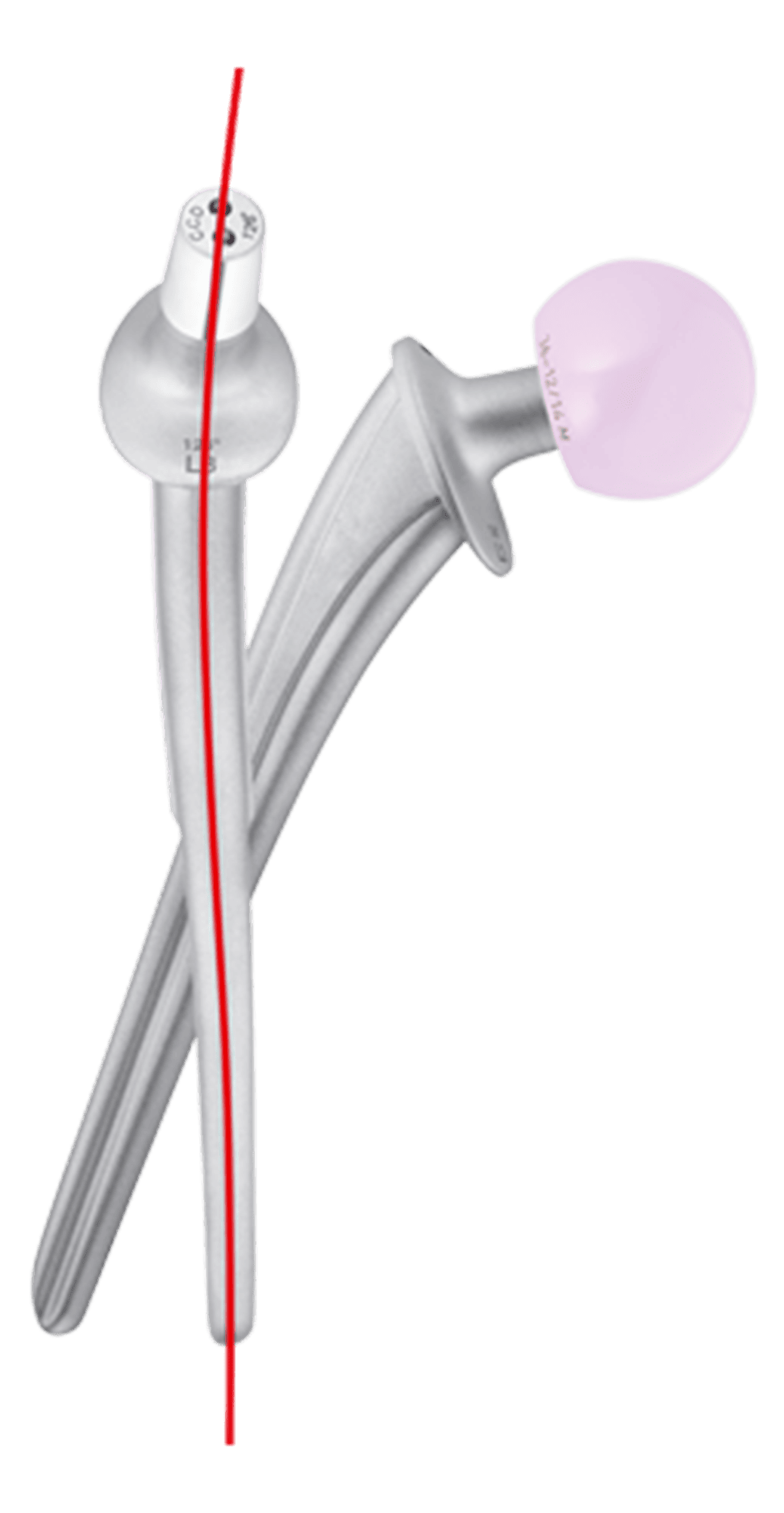
Mit der Entwicklung der zementfreien Version SP-CL hat LINK dieses Prothesensystem auf das nächste Level gebracht.
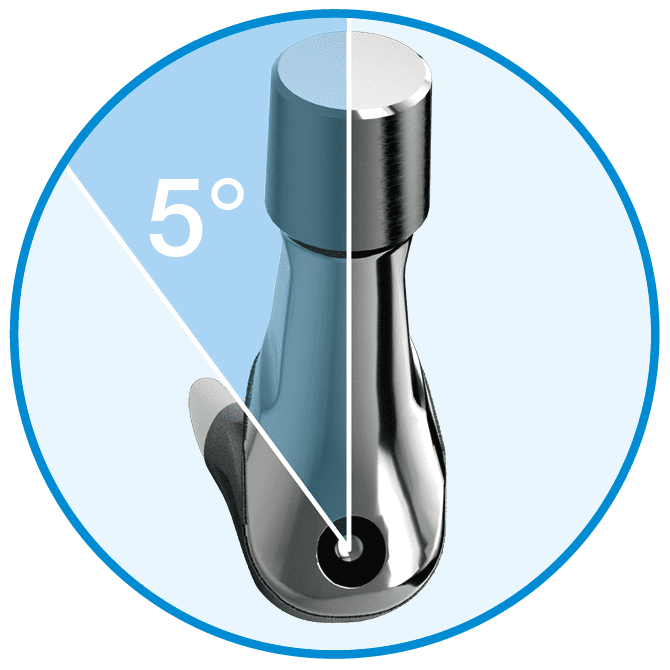
Wir haben klinisch bewährte Designmerkmale der zementierten SPII Prothese an die Anforderungen eines zementfreien Hüftschafts angepasst und so ein harmonisches Prothesensystem nach dem Prinzip „Die Anatomie bestimmt die Form“ geschaffen.
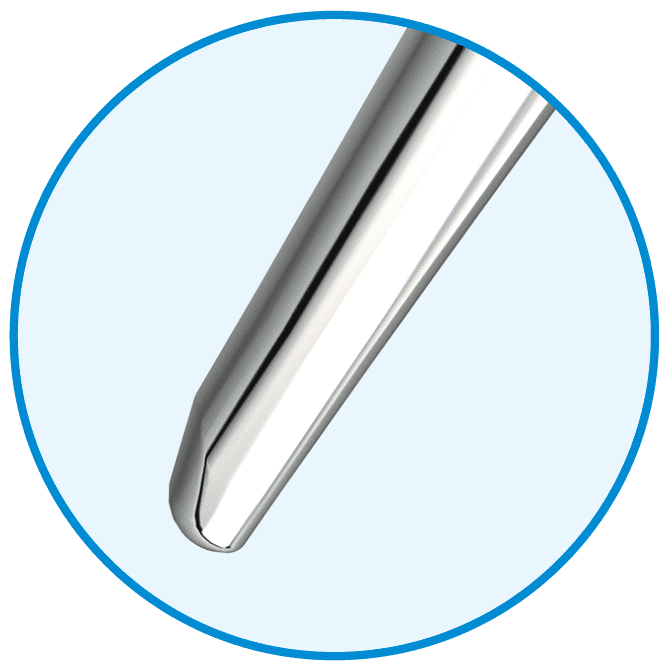
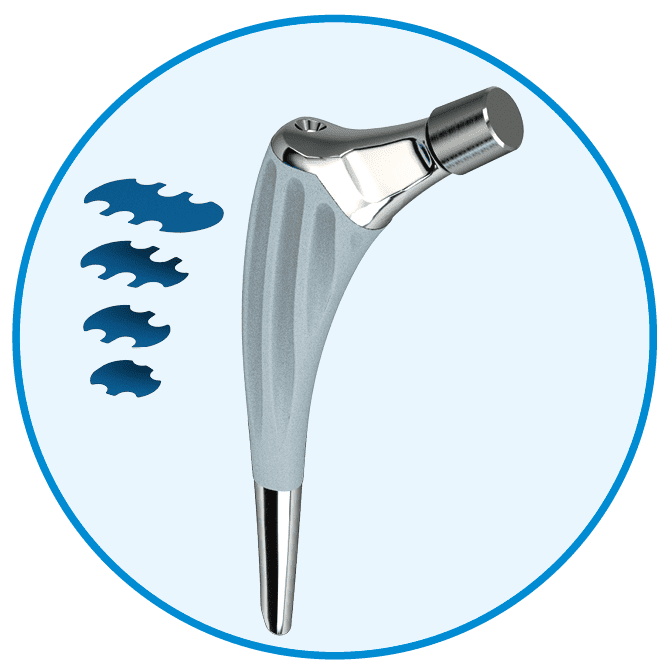
Während das spezielle Implantatdesign Knochen und Weichgewebe erhält3, erlaubt das umfassende Implantatsortiment die individuelle Anpassung an die Anatomie der Patienten. 4
Ergänzt wird das System durch ein kompaktes, ergonomisches Instrumentarium für einen reibungslosen und effizienten Gelenkersatz. 3



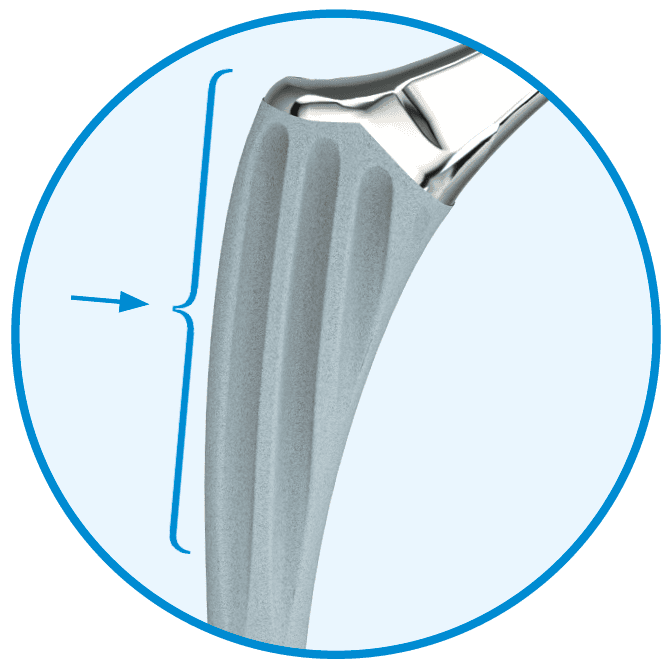
Hohe Primärstabilität und reduziertes Stress-Shielding
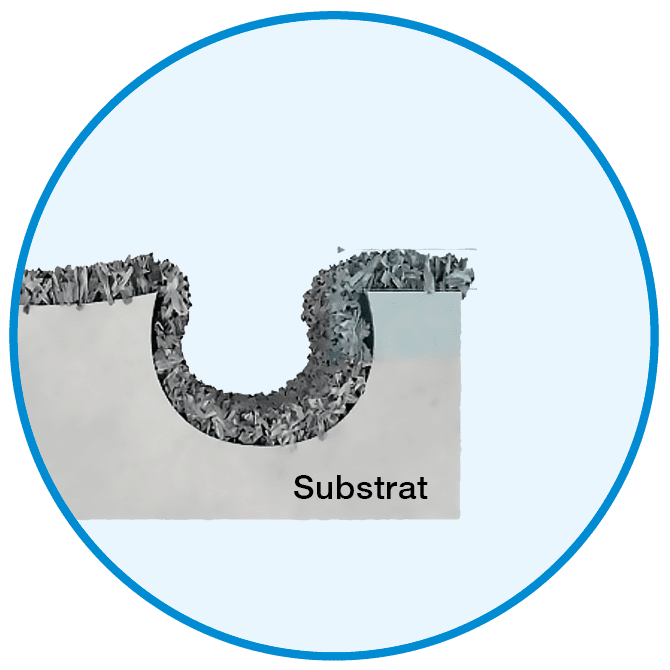
Durch die klinisch erprobte Rippenstruktur wird der Schaft in der komprimierten Spongiosa verankert und
eine hohe Primärstabilität sichergestellt. 6, 11, 12
In Kombination mit der LINK Tilastan-S Legierung wird die bekannte Elastizität des Materials selbst insbesondere durch die strukturelle Elastizität des Schaftdesigns unterstützt, um Stress-Shielding zu reduzieren.5, 6







Quellen
- W.T. Stillwell. (1987). The Art of Total Hip Arthroplasty. Grune & Stratton, pp. 296.
- Annual Report 2016; Swedish Hip Arthroplasty Register; www.shpr.se.
- Internes Dokument W. Link
- Vidalain, J. P., et al. (2011). The Corail Hip System. A practical approach based on 25 years of experience. Springer Heidelberg. pp. 54.
- Pipino, F., Keller, A. (2006). Tissue-sparing surgery: 25 years’ experience with femoral neck preserving hip arthroplasty. Journal of Orthopaedics and Traumatology, 7(1), pp. 36-41.
- Langhans, M., Hofman, D., Ecke, H., & Nietert, M. (1992). Der Einfl uß der Formgebung des Prothesenschaftes auf die Beanspruchung des proximalen Femurs. Unfallchirurgie, 18(5), pp. 266-273.
- Noble, P., Alexander, J., Lindahl, L., Yew, D., Granberry, W., & Tullos, H. (1988). The anatomic basis of femoral component design. Clinical Orthopaedics and Related Research (235), pp. 148-165.
- Denaro, V., & Fornasier, V. (2000). Fill, fi t and conformation - an anatomical and morphometric study of a hip component in total hip arthroplasty (Rippen-Link). European Journal of Orthopaedic Surgery & Traumatology, 10(4), pp. 239-247.
- Palm, L., Jacobsson, S., & Ivarsson, I. (2002). Hydroxyapatite coating improves 8- to 10-year performance of the link RS cementless femoral stem. The Journal of Arthroplasty, 17(2), pp. 172-175.
- DiGiovanni, C.W., Garvin, K.L., Pellicci, P.M. (1999). Femoral preparation in cemented total hip arthroplasty: reaming or broaching? Journal of the American Academy of Orthopaedic Surgeons, 7(6), pp.349-357.
- Schill S, Thabe H. (2000). Long- and Mid-Term Results of the Cementless Link Prosthetic System in Combination with the Ribbed Stem and Screw-in Cup, Type “V”. Orthopädische Praxis, 36, pp. 160-167.
- Thabe H, Wolfram U, Schill S. (1993). Medium-term results using the cement-free link endoprosthesis. Ribbed shaft V socket. Zeitschrift fur Orthopädie und ihre Grenzgebiete, 131(6), pp. 568-573.
- Petrou, G., Gavras, M., Diamantopoulos, M., Kapetsis, T., Kremmydas, N., & Kouzoupis, A. (1994). Uncemented total hip replacements and thigh pain. Archives of Orthopaedic and Trauma Surgery, 113(6), pp. 322-326.
- Khanuja, H., Vakil, J., Goddard, M., & Mont, M. (2011). Cementless femoral fi xation in total hip arthroplasty. The Journal of Bone & Joint Surgery, 93(5), pp. 500-509.