35 Years, One Implant: A Milestone in Oncologic Arthroplasty
After Tibial Sarcoma Resection: 35-Year Survivorship of a Cemented Custom Rotating Hinge Knee Prosthesis
Arthroplasty following tumor resection in young patients is a demanding clinical scenario due to their high functional requirements and long life expectancy. Cemented knee prostheses are frequently regarded as too aggressive for this population. This case report presents an exceptional 35-year outcome following implantation of a cemented, custom-made rotating hinge knee prosthesis after tibial sarcoma resection in a young female patient.

Figure 1: Preoperative full-length AP X-ray showing the original cemented custom-made knee prosthesis 35 years after implantation
Initial Reconstruction and Long-Term Clinical Course
In 1990, a 23-year-old female patient underwent resection of a tibial sarcoma and received a cemented, custom-made Endo-Model Rotating Hinge Knee prosthesis from LINK. The prosthesis was implanted in Hospital Sant Pau in Barcelona, Spain, by Dr. Joan Majó. The original long tibial component with allograft reconstruction was left in situ. For the subsequent 35 years, the implant maintained full functionality, with no requirement for surgical intervention. At the time of implantation, many proponents of conservative implant strategies would have considered a cemented hinge knee prosthesis too aggressive for a 23-year-old patient.
The patient recently presented with mechanical symptoms due to failure of the T-bushing in the femoral component. During the revision surgery, the femoral component of the prosthesis was extracted and substituted with a modular Endo-Model Rotating Hinge Knee femoral component and a TrabecuLink FlexiCone from LINK. To optimize the mechanical function of the new T-bushing, the femur was slightly distalized. The original tibial component, inclusive of the allograft, was securely fixed and left in place. The surgical revision was carried out by Dr. Isidre Gracia at Hospital Sant Pau in Barcelona, Spain.
Reevaluating Cemented Hinge Arthroplasty in Young Patients
Initial Reconstruction and Long-Term Clinical Course
This case presents a challenge to the prevailing notion that cemented knee prostheses are inherently unsuitable for young patients. Notwithstanding the patient's youth at the time of surgery and the complexity of the initial reconstruction, the prosthesis functioned reliably for 35 years without requiring revision. The incorporation of the contemporary TrabecuLink FlexiCone component from LINK exemplifies the adaptability of contemporary implant technologies, even in the context of integrating them into existing systems. This outcome supports the long-term viability of cemented custom prostheses in oncologic arthroplasty and emphasizes the importance of individualized treatment planning over rigid adherence to surgical doctrine.
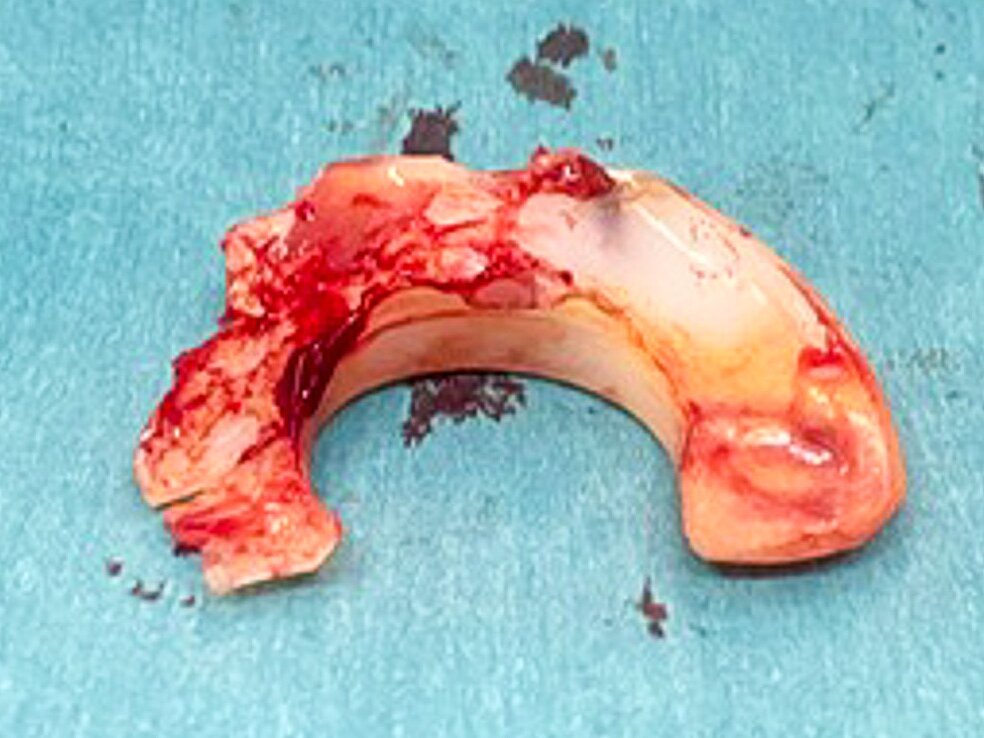
Figure 2: Explant of the fractured polyethylene T-bushing, showing material degradation and mechanical wear after 35 years of in vivo function in a rotating hinge knee prosthesis.

Figure 3: New polyethylene T-bushing (LINK) prepared for implantation.
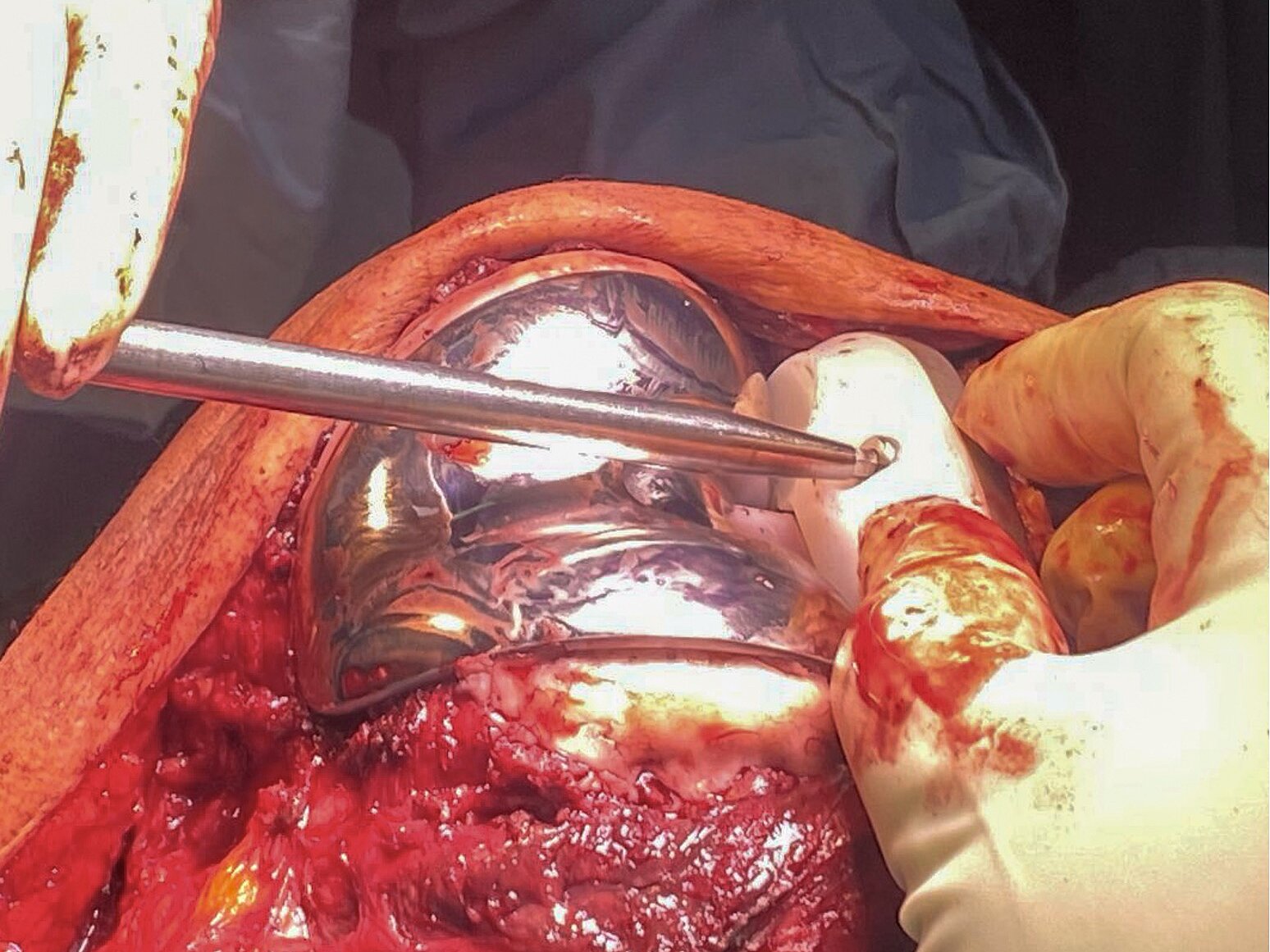
Figure 4: Intraoperative photograph showing removal of the original femoral component using a dedicated extraction instrument. The tibial component and allograft remain undisturbed in situ.
Conclusion

Figure 5: Postoperative X-rays, anteroposterior view (left), lateral view (right).

This case demonstrates that a cemented custom knee prosthesis can provide excellent long-term function and stability in a young patient following tumor resection. In instances where revision becomes necessary, modern components such as the Trabeculink FlexiCone from LINK can be incorporated with success without compromising the original reconstruction. The findings of this case provide further evidence in support of the efficacy of durable primary solutions in the field of oncologic arthroplasty, as demonstrated by the long-term follow-up results.

Figure 6: Intraoperative fluoroscopy (anteroposterior view) after femoral revision. The TrabecuLink FlexiCone femoral component articulates with the preserved tibial stem. Correct alignment and articulation are confirmed.