Reconstructing Stability: Salvage Reconstruction After Failed Two-Stage Exchange in Chronic Multidrug-Resistant Hip Infection
Early User Experience with the MobileLink PPR by Dr. Sanz-Ruiz, Madrid, Spain
Chronic periprosthetic joint infection (PJI) caused by multidrug-resistant organisms remains one of the most demanding challenges
in revision hip arthroplasty. When multiple debridements and even a two-stage exchange fail, the problem becomes both biological
and mechanical. Infection control must be re-established while simultaneously addressing bone loss, instability, and compromised
soft tissues. This case illustrates how infection eradication and biomechanically coherent reconstruction were combined to restore
function in a multiply operated hip with complete posterior wall deficiency and severe acetabular bone loss.
Background and Clinical Presentation

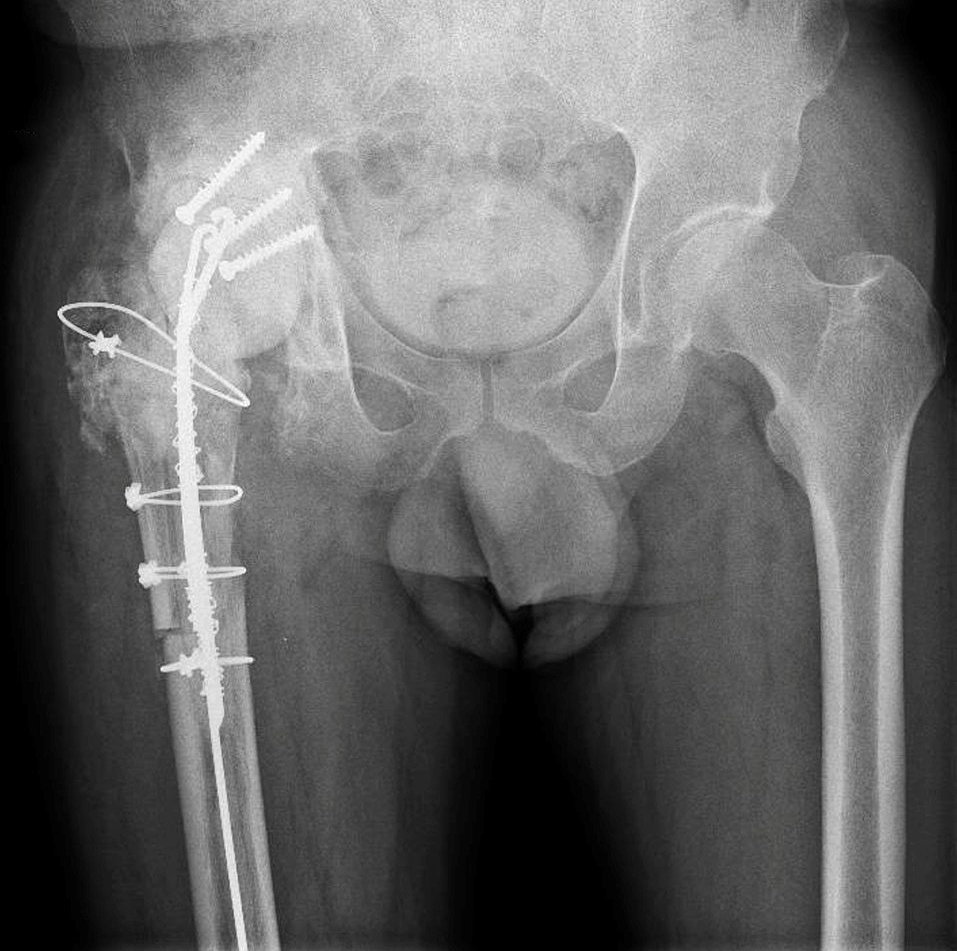
Preoperative X-ray demonstrating severe acetabular bone loss and loosening in a multiply revised right hip.
A 64-year-old male patient with arterial hypertension and no known drug allergies was referred with chronic PJI of the right hip
due to multidrug-resistant Pseudomonas aeruginosa.
His surgical history was complex. Thirty years earlier, he had sustained an acetabular fracture in a road traffic accident that had
been treated with osteosynthesis. This was followed by total hip arthroplasty for post-traumatic osteoarthritis and an early acetabular revision two years later. Subsequently, he developed a PJI that had already been treated with a two-stage exchange. Despite repeated debridements, the infection persisted.
At presentation, clinical examination revealed multiple lateral and posterolateral scars, a proximal fistula with seropurulent discharge, and severely restricted range of motion limited to 0–45° of flexion with absent rotations.
Plain radiographs demonstrated a loose acetabular component, severe acetabular bone loss, and heterotopic ossification.
First Stage: Explantation and Spacer Strategy
First-stage reconstruction with antibiotic-loaded spacer and temporary posterior wall reconstruction (tectoplasty) using bone cement reinforced with screw fixation.
Given the presence of a difficult-to-treat microorganism and previous failure, a repeat two-stage exchange was
indicated.
Through a posterolateral approach, implant removal was performed. Because of limited exposure and the risk of
fracturing the remaining trochanteric bone, an extended trochanteric osteotomy was required to gain adequate access to the acetabulum.
After complete implant removal, thorough surgical, mechanical, and chemical debridement was carried out.
A hand-made spacer was implanted using COPAL G+C cement. Each cement package was additionally loaded
with 2g of meropenem and 2 million IU of colistin to achieve high local antibiotic concentrations.
A particular challenge was the complete absence of the posterior wall, secondary to the old acetabular fracture. To provide containment and prevent spacer instability, a tectoplasty was performed using bone cement reinforced with three screws to reconstruct a temporary posterior wall and stabilize the spacer.
The patient underwent six weeks of targeted antibiotic therapy. After normalization of inflammatory markers and
adequate wound healing, reimplantation was scheduled.
Second Stage: Addressing Multidirectional Instability
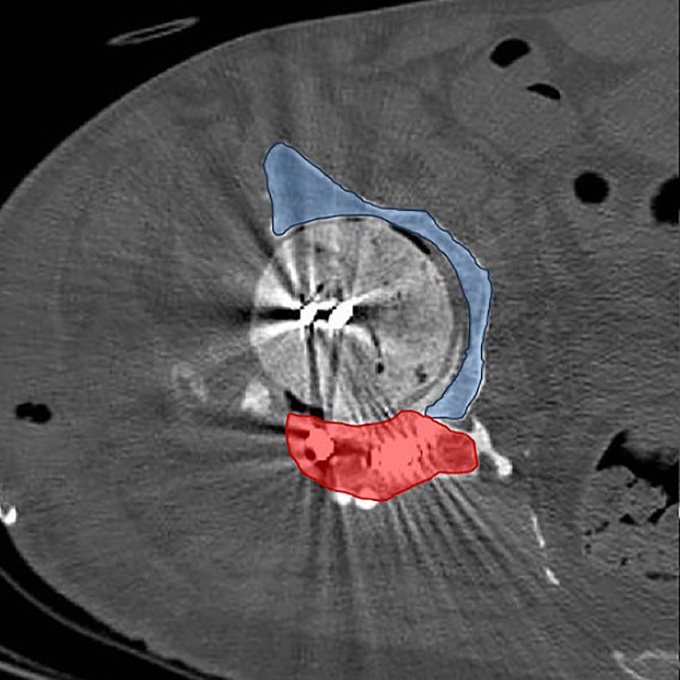
Axial CT image illustrating temporary posterior wall (red) and residual bone stock (blue), explaining multidirectional instability.
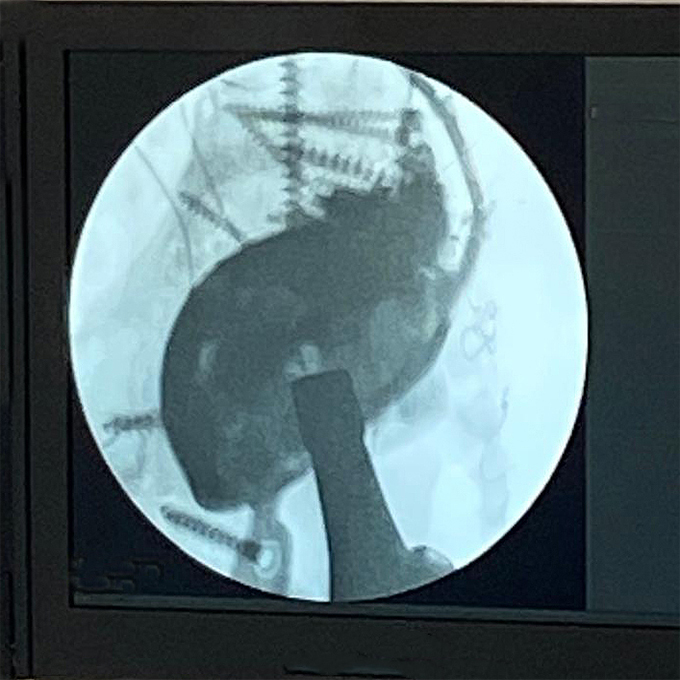
Intraoperative fluoroscopic assessment during definitive reconstruction.
During reimplantation, removal of the spacer and prior tectoplasty exposed a Paprosky IIIA acetabular defect. A complete posterior wall deficiency combined with a significant superior acetabular roof defect resulted in translational instability of the trial component in both cranio-caudal and anteroposterior directions. Cranio-caudal stability was achieved using a cranial trabecular titanium augment (TrabecuLink Augments). However, anteroposterior instability persisted.
The decisive step in reconstruction was the mechanical integration of a PPR-type acetabular cage with the trabecular titanium augment. The flanges of the MobileLink PPR were connected directly to the augment using 4.5 mm screws, transforming two independent components into a unified structural construct.
This integrated configuration restored stability in both planes and allowed early full weight-bearing.
On the femoral side, a LINK MP stem combined with an MP 2.0 metaphyseal component (38 mm offset) was implanted. Given the multiply operated hip and compromised soft tissues, a dual mobility articulation (MobileLink Dual Mobility Insert) with ceramic head was chosen to reduce dislocation risk.
Outcome and Discussion
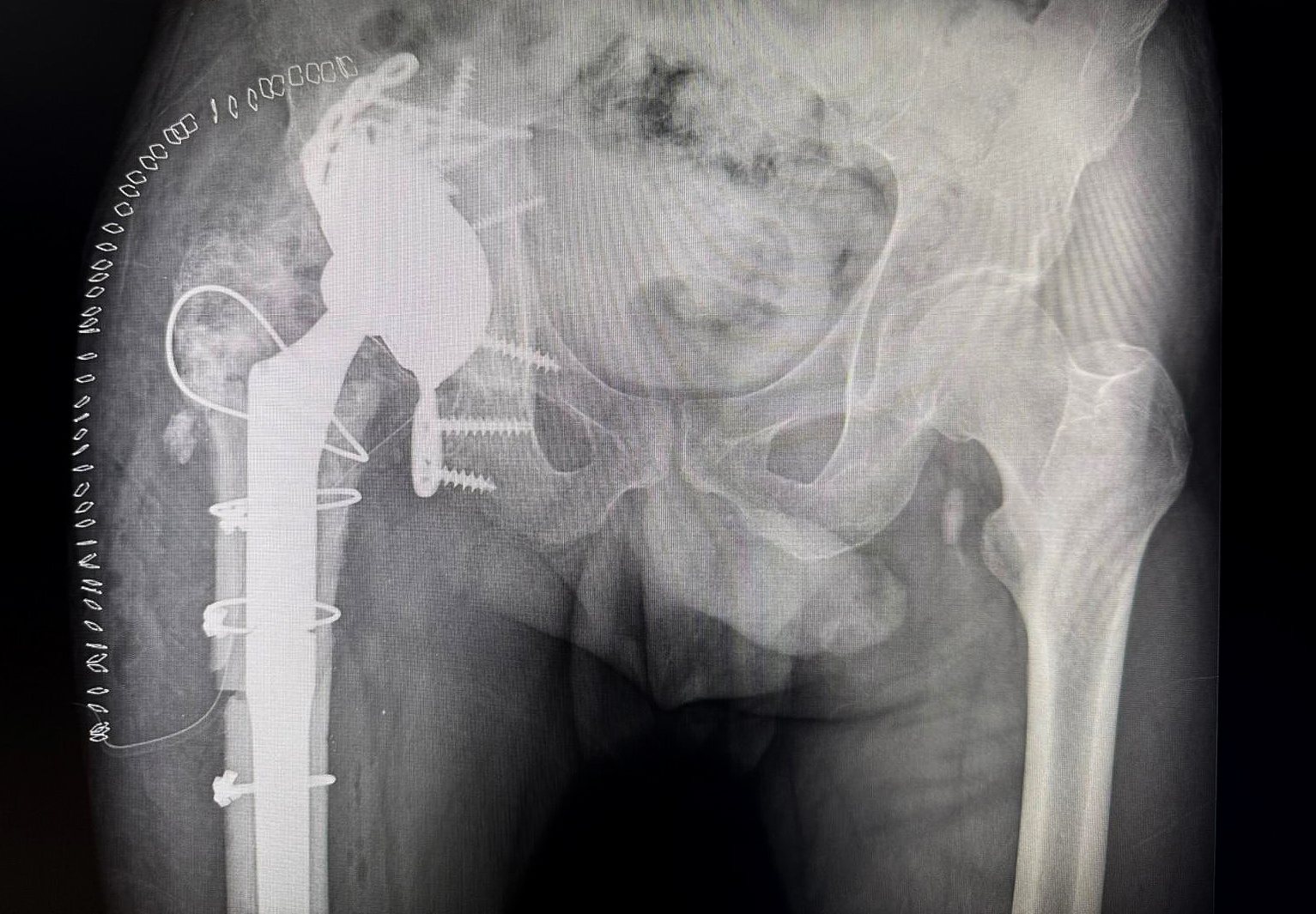
Postoperative X-ray showing integrated augment–cage construct with stable fixation, allowing early full weight-bearing.
The extreme malleable flanges allowed the cranial fixation.
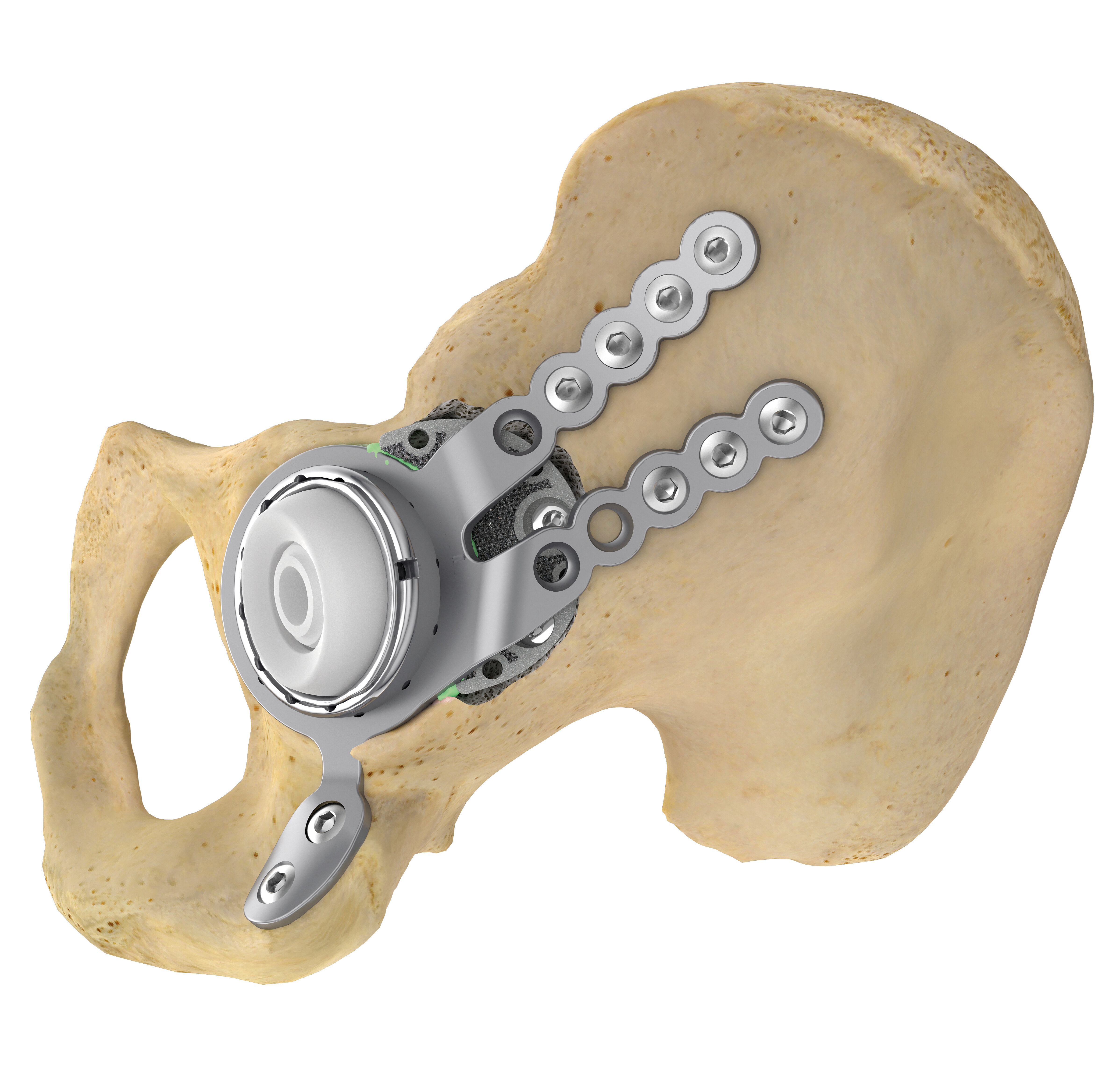
Off-the-shelf MobileLink PPR using a Dual Mobility Insert, combined with a TrabecuLink Augment.
At 18 months follow-up, the patient remains asymptomatic. He ambulates without walking aids and demonstrates active hip flexion of 90 degrees. There are no clinical or laboratory signs of recurrent infection.
This case highlights the dual challenge inherent to chronic multidrug-resistant PJI in the presence of severe acetabular bone loss. Biological eradication of infection required aggressive debridement and high-dose local antibiotic delivery. Mechanical reconstruction required understanding the biomechanics of the defect rather than relying solely on classification.
The absence of the posterior wall created anteroposterior instability that could not be resolved by cranial augmentation alone. By mechanically linking a trabecular titanium augment to a PPR cage, structural logic was restored. Stability was achieved not through implant complexity but through coherent construct integration. In multiply revised hips, dual mobility articulation adds an additional layer of safety by reducing dislocation risk in compromised soft tissue environments.
Ultimately, successful salvage revision depends on addressing infection control and structural reconstruction simultaneously. When both are conceptually aligned, even severely compromised hips can regain function and durability.