Rebuilding the Shoulder: Custom Total Scapula Replacement After High-Grade Osteosarcoma
Malignant tumors of the scapula represent one of the most demanding scenarios in musculoskeletal oncology. When a high-grade osteosarcoma involves the entire scapular body, surgery requires not only oncologic precision but also a sophisticated reconstructive strategy. The removal of the scapula eliminates a key structural and biomechanical element of the shoulder girdle. Without reconstruction, the patient would be left with profound instability and severely compromised upper limb function.
This case demonstrates how a patient-specific total scapula replacement enabled stable anatomical reconstruction and functional restoration following complete tumor resection.
Preoperative Situation
The patient, over 35 years of age and taller than 160 cm, was diagnosed with a high-grade osteosarcoma of the left scapula. Preoperative imaging revealed extensive tumor involvement of the scapular body, making partial resection oncologically unsafe. A total scapulectomy was therefore indicated.
The clinical challenge extended far beyond tumor removal. The scapula serves as the anchoring platform for multiple muscle groups and provides the foundation for glenohumeral articulation. Its loss disrupts load transfer, alters the center of rotation, and compromises shoulder stability. The reconstructive objective was therefore to re-establish a stable articulation, allow reliable soft-tissue reattachment, and optimize biomechanical balance while maintaining oncologic safety.
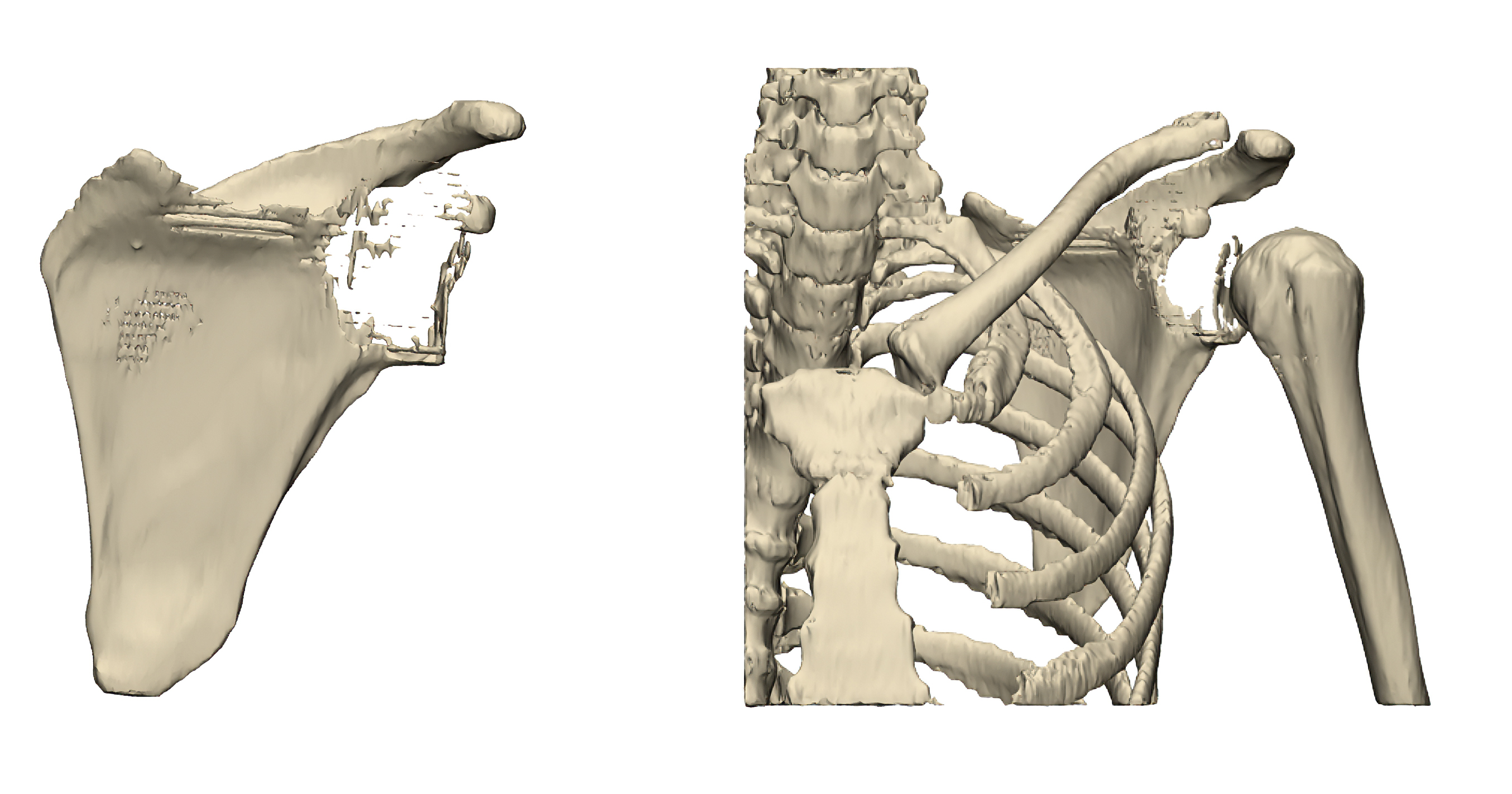
Preoperative 3D reconstruction demonstrating extensive tumor involvement of the left scapula.
Resection Planning

Oncologic resection planning with preservation of the proximal humerus.
The surgical plan followed established oncologic principles, ensuring complete tumor removal with adequate margins while preserving the proximal humerus. Maintaining the humerus allowed for a reconstructive concept based on controlled articulation rather than amputation or purely palliative stabilization.
At this stage, it became clear that a standard implant system would not adequately address the complex anatomical and biomechanical requirements. A custom-engineered solution was necessary to recreate the structural framework of the scapula and integrate a functional shoulder articulation.
Patient-Specific Implant Design

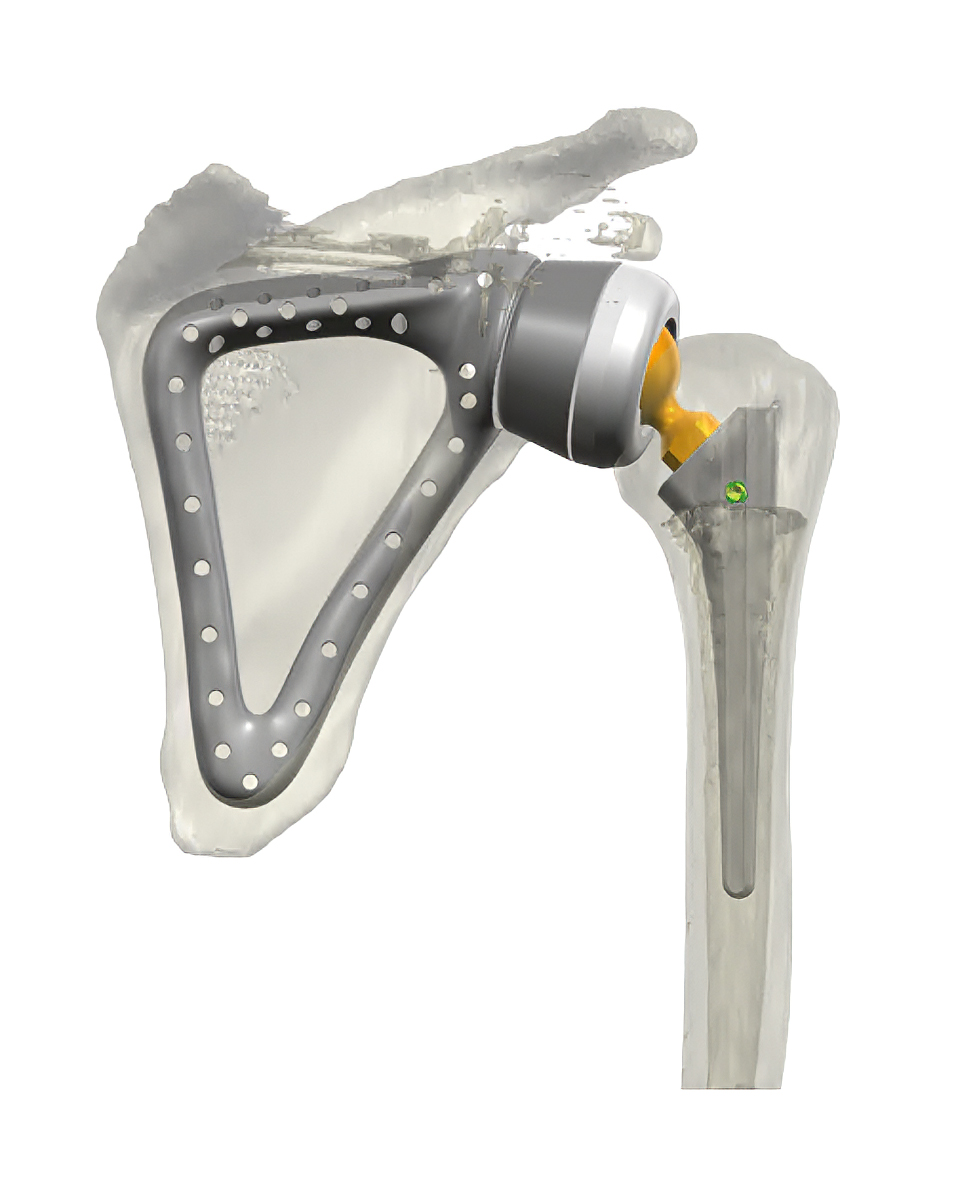
Patient-specific total scapula prosthesis (with custom humeral stem) designed for anatomical reconstruction and biomechanical restoration, prior to implantation
A fully customized total scapula prosthesis was developed based on the patient’s anatomy and the planned surgical resection. The design process focused on anatomical fidelity, mechanical stability, and soft-tissue integration.
The scapular body was reconstructed with an anatomy-matched geometry and advanced fixation concept. A central window concept reduced weight while preserving structural rigidity. Multiple suture holes were incorporated to facilitate systematic reattachment of muscles and soft tissues, a critical prerequisite for postoperative function and stability.
The glenoid articulation was addressed through a custom cup and insert, precisely adapted to the resection geometry and anchoring requirements. A custom-designed head with screw fixation provided a secure mechanical interface to the humeral component. The custom humeral stem, cemented and based on established Embrace shoulder system geometry, ensured reliable fixation within the preserved humeral shaft.
Particular attention was paid to biomechanical optimization. The center of rotation and humeral neck length were carefully adjusted to restore balanced load distribution and improve functional potential.
Implantation and Postoperative Outcome
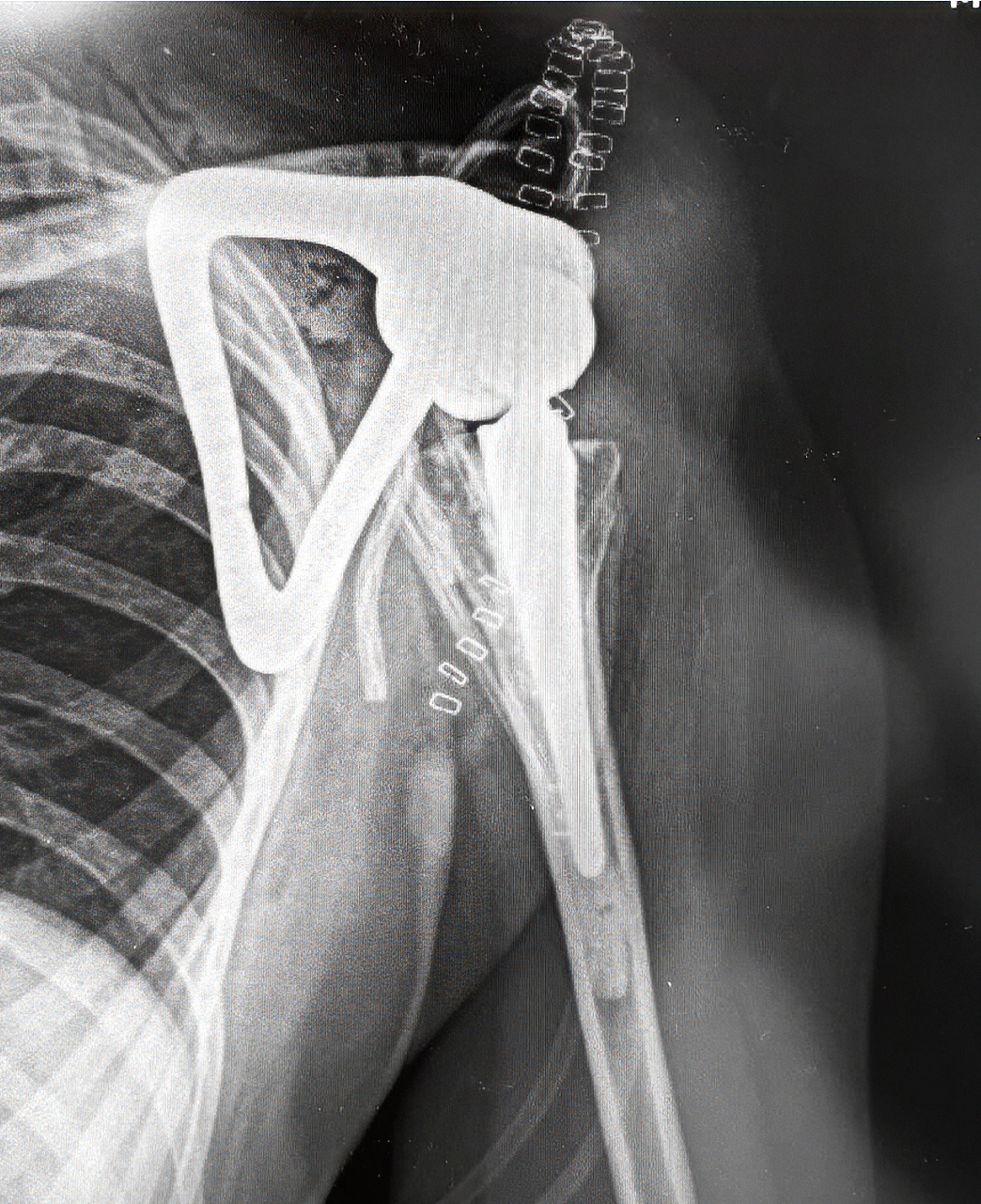
Postoperative radiograph confirming stable reconstruction and anatomical alignment.
Following complete tumor resection, the custom scapula prosthesis was implanted according to the preoperative plan. Postoperative X-rays confirm stable positioning and correct alignment of the reconstruction. The anatomical relationship between the custom scapular body and the humeral component demonstrates precise execution of the surgical and engineering concept.
The reconstruction achieved structural stability and provided a defined articulation, creating the basis for functional recovery. Most importantly, the implant design allowed systematic soft-tissue reattachment, which is indispensable for long-term shoulder function in total scapula replacement cases.
Through meticulous interdisciplinary planning and individualized implant engineering, limb preservation was achieved while restoring upper limb stability and mobility.
Conclusion
Total scapula replacement represents one of the most complex reconstructive challenges in orthopedic oncology. Standardized implant systems often cannot meet the anatomical
and biomechanical demands following complete scapulectomy.
In this case, a patient-specific custom solution enabled anatomical reconstruction, biomechanical optimization, and stable fixation within an oncologically safe framework. The result
underscores the importance of customized implant design when standard solutions reach their limits.