MEGASYSTEM-C in Oncologic and Complex Revision Surgery: Clinical Experience, Customization Strategies, and Infection Management
In October 2025, LINK had the pleasure of welcoming Prof. Domenico Andrea Campanacci and Prof. Davide Maria Donati to our headquarters in Hamburg and our production site in Norderstedt.
During their two-day visit, we recorded three expert interviews discussing the clinical application of MEGASYSTEM-C in complex oncologic reconstructions, septic revisions, and catastrophic bone loss cases. The conversations offer valuable insights into modular precision, custom solutions, and infection management from two leading specialists in orthopedic oncology.
In this LINK Expert Dialogue, Prof. Campanacci and Prof. Donati reflect on more than two decades of experience with the MEGASYSTEM-C in orthopedic oncology and complex reconstructive surgery.
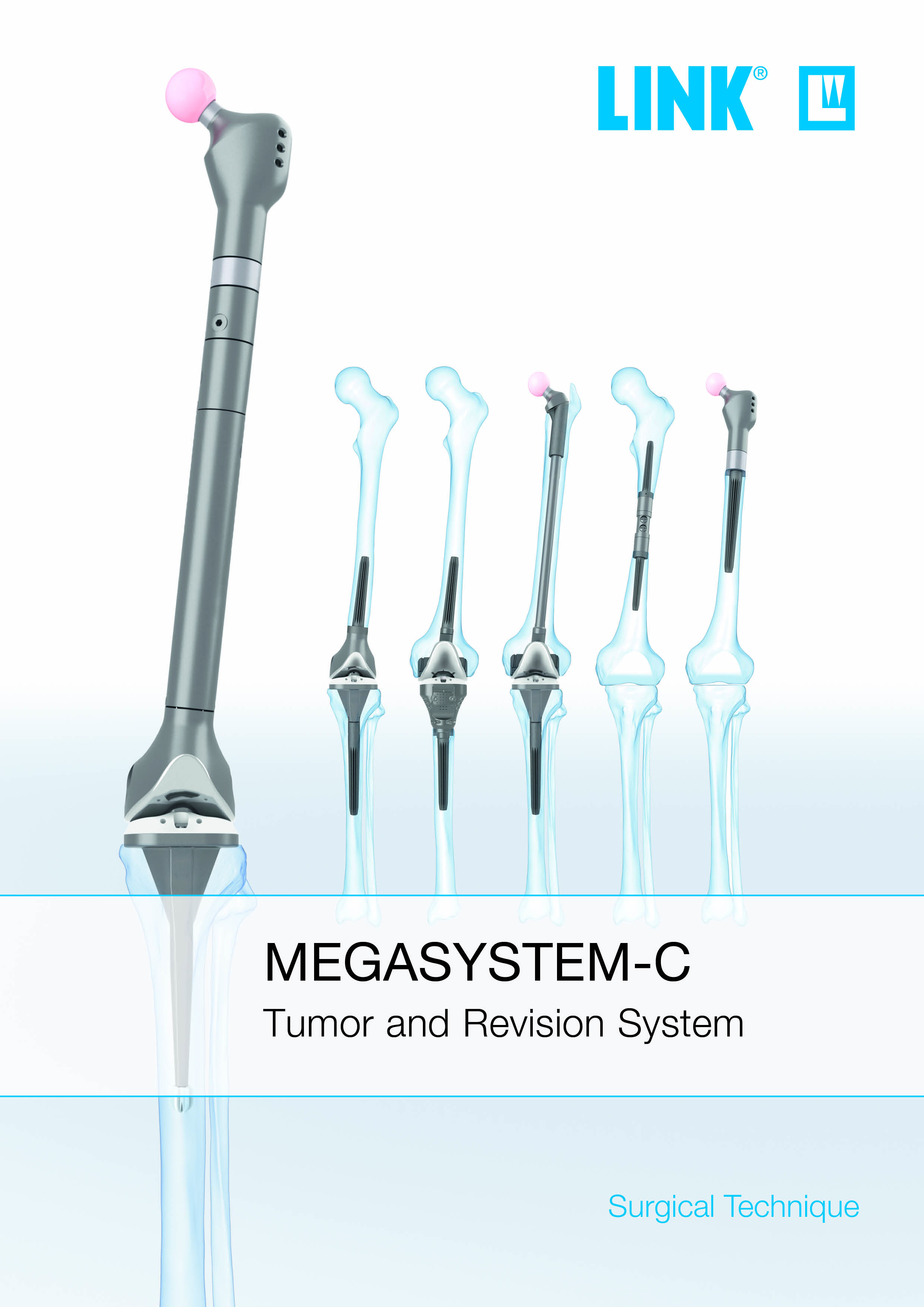
Originally developed for oncologic reconstruction, the system has become
a cornerstone of managing extensive bone loss due to primary tumors, metastases, major post-traumatic defects, and complex prosthetic revisions.
Discover the key takeaways in the abstract below
and watch the full expert interviews in the linked videos...
Prof. Campanacci outlines the challenges of pelvic and sacroiliac tumor resections, where complex three-dimensional anatomy and proximity to critical neurovascular structures demand advanced expertise. In extensive defects, intraoperative navigation and CT-based 3D imaging are essential for accurate resection and implant positioning. Custom-made implants are indispensable when reconstructing the entire hemipelvis or when pelvic resection must be combined with total femoral replacement—among the most demanding procedures in orthopedic oncology.
Prof. Donati presents a salvage case involving an elderly patient after third revision of an infected knee prosthesis. Following arthrodesis and subsequent periprosthetic femoral fractures, a total femoral replacement using a push-through megaprosthesis preserved the trochanter and hip joint. At two-year follow-up, the outcome was satisfactory despite permanent knee arthrodesis, illustrating the system’s role in catastrophic septic failure.
Prof. Campanacci and Prof. Donati both emphasize that megaprosthetic surgery requires specialized training, with oncologic resection preceding reconstruction. The system’s application has expanded beyond tumor surgery into complex revision arthroplasty.
Future challenges include improving soft-tissue reinsertion, enhancing long-term stem stability to reduce aseptic loosening, and advancing infection prevention. Continuous collaboration between surgeons and engineers is essential for further refinement of implant design and surface technologies.
The MEGASYSTEM-C is thus viewed as an evolving reconstructive platform that integrates modular
precision, patient-specific customization, and technological innovation to address the most demanding scenarios in contemporary orthopedic surgery.
A central strength of MEGASYSTEM-C is its modularity. Centimeter-by-centimeter adjustment allows precise limb-length restoration, while rotational alignment and anteversion can be refined even after stem implantation. The system integrates with structural bone grafts and composite techniques. Custom components further expand options in anatomically challenging regions such as the pelvis, shoulder girdle, talus, and calcaneus, and enable fixation in cases with very short residual bone segments, including joint-sparing reconstructions. In revision surgery, retaining well-fixed components may reduce additional bone loss in selected elderly or osteoporotic patients. Custom connectors can integrate preserved modular parts, avoiding unnecessary removal of stable integrated implant components.
Infection remains one of the most serious complications, particularly in oncologic patients receiving chemotherapy. Both surgeons advocate two-stage revision as the most reliable strategy in chronic or severe infection. In selected high-risk patients, partial retention strategies may prevent excessive bone loss. In specialized centers, megaprosthetic reconstruction after major infection—combined with anti-infective measures such as silver surface treatment (PorAg)—can achieve success rates of approximately 80–85%.
Surface technologies are considered critical for future development. PorEx is used in patients with metal hypersensitivity. Hydroxyapatite coatings enhance osseointegration, particularly at stem collars. PorAg silver coatings may reduce infectious risk in septic revisions, although definitive evidence remains under evaluation.