

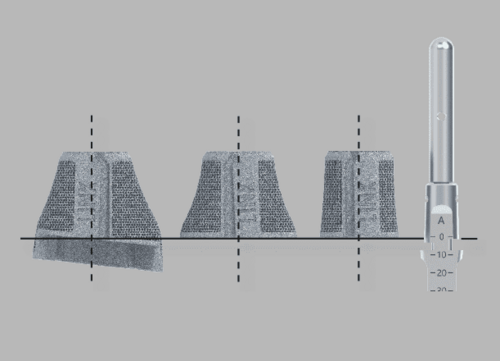
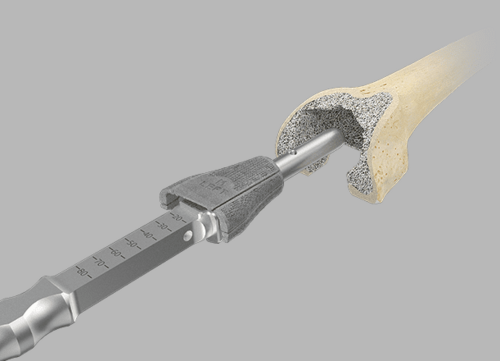
The zero position on the scale marked on the impactor indicates the level of the Femoral Cone/intracondylar box of Endo-Model femoral components.
- Safety:
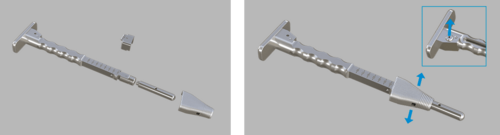
- Adapters can only be assembled in one direction in relation to the femoral impactor
- An integrated magnet in the femoral impactor helps in attaching the adapter in the correct position
- One-hand technique: The button on the rear of the impactor must be depressed and held down to attach the femoral compressor or final implant with the other free hand
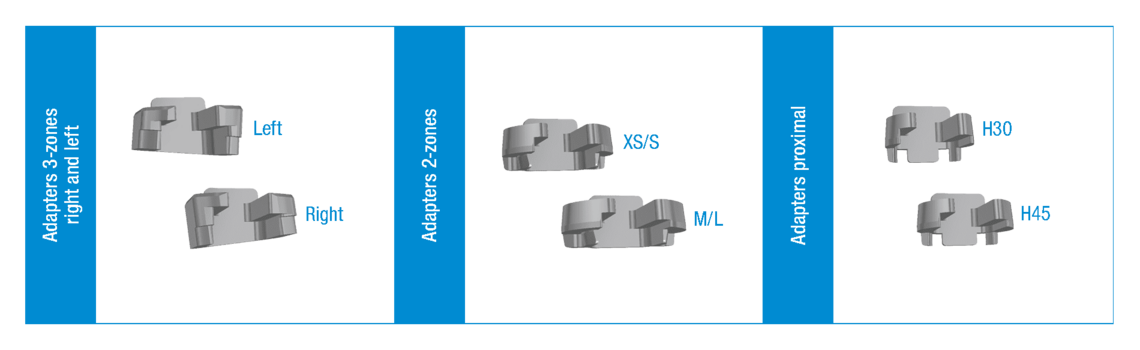
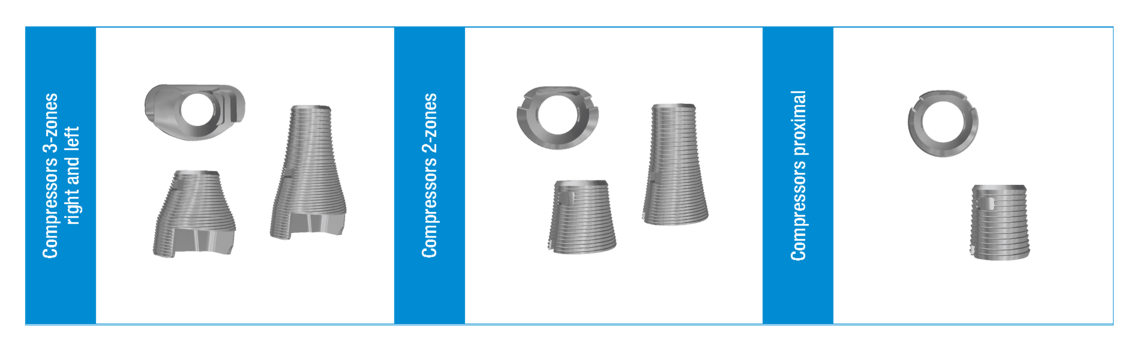
Double-check the correct choice of adapter, especially when using 2-zone or 3-zone cones. The laser marking is as follows (left/right or XS/S or H30/ H45)
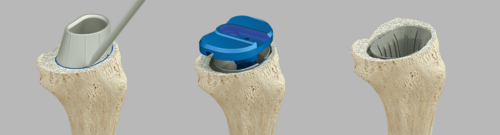
The Femoral Compressors have 2 functions. They serve as a rasp and as a trial implant. In order to check that the fit is correct, it is necessary to carry out a trial reduction with all the trial components from the Endo-Model Knee Family. After trial reduction, it may be advantageous to leave the femoral compressor in situ until shortly before implantation of the final implant.
Filling outer spaces Once the Femoral Cone has been placed, any spaces at the implant/bone interface can be filled with autologous material in order to achieve additional stability and prevent undesirable flow of cement between implant and bone.
Please note: Another option is to fill any outer spaces with bone graft material and compress
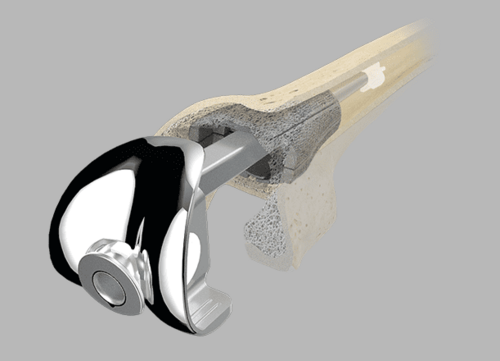
After implantation of the final Femoral Cone implant, it is recommended to double-check that it is correctly seated before placing the bone cement to fill the inner cavity.
This can be done with either the fully assembled femoral component (in the case of modular implant systems) or the femoral trial component. The purpose of the repeat trial, especially when using the 3-zone Femoral Cones, is to provide an intraoperative check for the appropriate box level between Femoral Cone and femoral knee component.
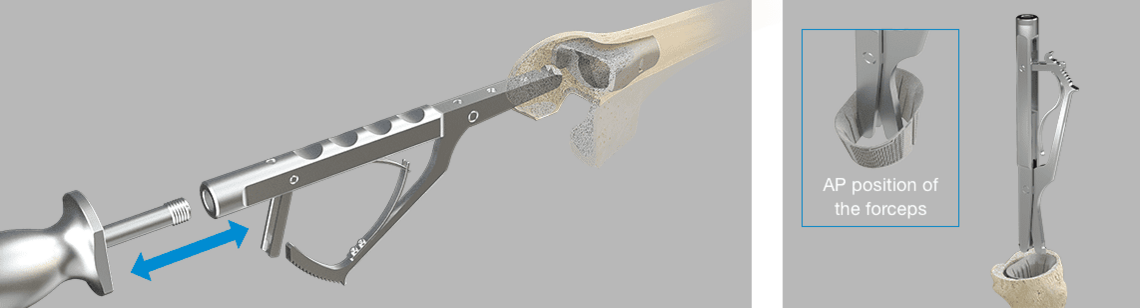
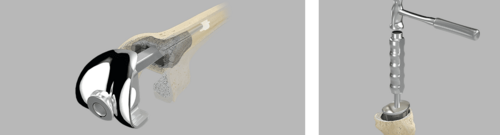
If it is necessary to reposition or explant the Femoral or Tibial Cone, the respective extraction forceps can be used after releasing the bony connection and removing the bone cement. In the event of a revision, both extraction forceps, i.e. for Femoral Cones or Tibial Cones, can be connected to the M12 thread of the forceps with a slap hammer.
After intramedullary insertion, the forceps grab underneath the cone rim. Repositioning of a Femoral Cone can also be done with the femoral impactor (see Tip 2).
Tibial Cones provide the same approach via the tibial trial cone.A reversed trial cone can be used to determine the version and size of Tibial Cone that needs to be inserted.
Another option is to fill and compress any outer spaces with bone graft material after placing the trial cone in trial positioning or repeat trial situations. After implantation of the final implant, it can again be advantageous to double-check that it is correctly seated before placing the bone cement to fill the inner cavity.
To prevent metal contact, it is recommended to make sure that the implant finishes somewhat distally below or proximally above (approx. 1 mm) the resection level.
When the Femoral Cone is implanted, its final seating should be approx. 1-2 mm ventral to the planned position of the intramedullary box.

TrabecuLink Cones: Biomechanical Analysis of TrabecuLink Flexible Femoral Cones in Endo-Model Hinged Total Knee Arthroplasty
Prof. Bernardo Innocenti, PhD
Major Findings
- Flexible Cone reduces bone stress during implantation, lowering the risk of bone fracture;
- Flexible Cone better distributes stress over the bone, improving implant stability;
- Flexible Cone does not alter the implant performance obtained with the rigid cones;
- Flexible Cone guarantees the same negligible implant micromotions obtained with the use of rigid cones.
To receive the complete FEA paper in print or PDF version, please contact us at info-flexicones@linkhh.de
Comparative Biomechanical In Vitro Study of Different Modular Total Knee Arthroplasty Revision Stems With Bone Defects
Dario Guttowski, Dr Med a, *, Valerie Polster, Dipl -Ing b, Gerd Huber, Dr Ing b, MichaelM.Morlock,Prof Dr b, Klaus Püschel, Prof Dr Med c, Jakob Nüchtern, PD,DrMed a
Abstract
Background
The aim of this study is to investigate the effects of different stem lengths and types including cones on primary stability in revision total knee arthroplasty with different femoral bone defects and fixation methods in order to maximize bone preservation. It is hypothesized that longer stems provide little additional mechanical stability.
Methods
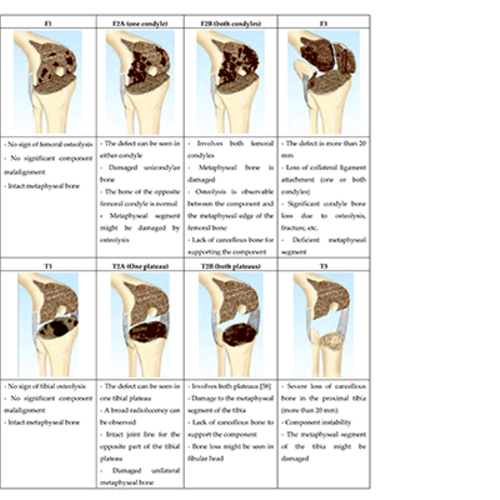
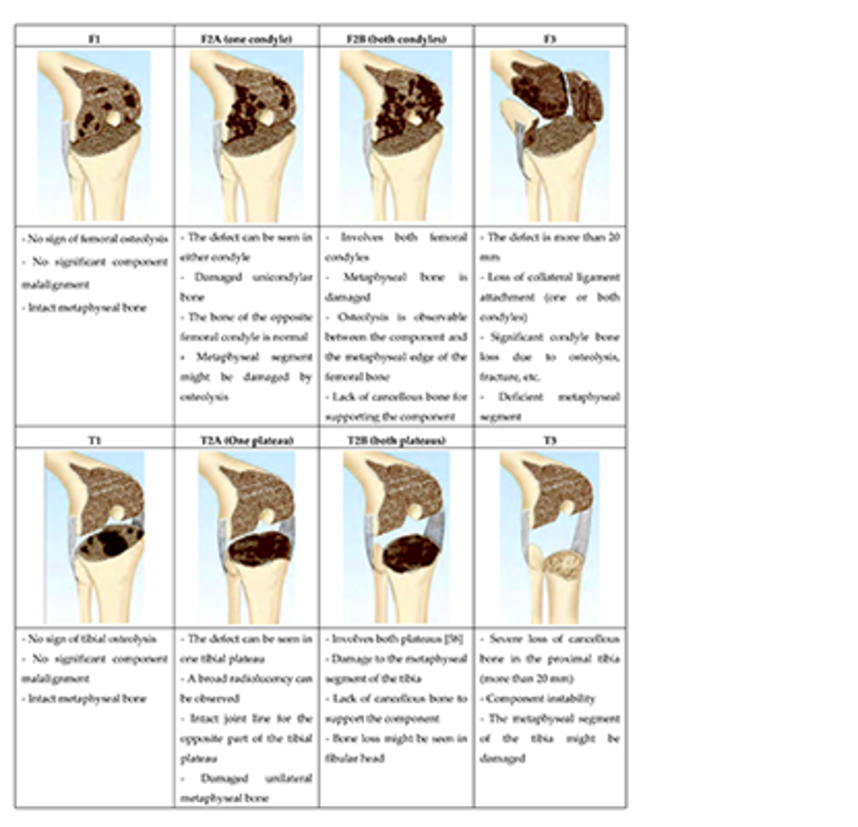
Thirty-five human femurs were investigated. A distal bone defect, Anderson Orthopedic Research Institute classification (s. 33) type-F2a, was created in group 1-3 and type-F3 in group 4-6. A cemented, rotating hinge femoral component was combined with different stems (100 and 160 mm total or hybrid cemented cones, or a 100-mm custom-made anatomical cone stem). The femora were loaded according to in vivo loading during gait. Relative movements were measured to investigate primary stability. Pull-out testing was used to obtain a parameter for the primary stability of the construct.
Results
Relative movements were small and similar in all groups (<40 μm). For small defect, the pull-out forces of cemented long (4583 N) and short stems (4650 N) were similar and about twice as high as those of uncemented stems (2221 N). For large defects, short cemented stems with cones showed the highest pull-out forces (5500 N). Long uncemented stems (3324 N) and anatomical cone stems (3990 N) showed similar pull-out forces.
Conclusion
All tested stems showed small relative movements. Long cemented stems show no advantages to short cemented stems in small bone defects. The use of cones or an anatomical cone stem with hybrid cementation seems to offer good stability even for larger bone defects. The use of a short cemented stem (with or without cone) may be a suitable choice with a high potential for bone preservation in total knee arthroplasty revision with respective bone defects.
Learn more here
PAPER R. MORGAN-JONES
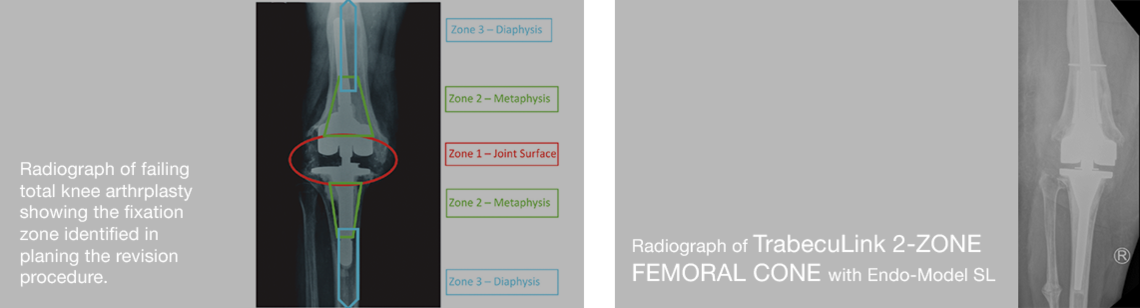
Zonal Fixation in revision total knee arthroplasty
Zonal fixation in revision total knee arthroplasty R Morgan-Jones, S I S Oussedik, H Graichen, F S Haddad Affiliations
PMID: 25628273 DOI: 10.1302/0301-620X.97B2.34144
Abstract
Revision knee arthroplasty presents a number of challenges, not least of which is obtaining solid primary fixation of implants into host bone. Three anatomical zones exist within both femur and tibia which can be used to support revision implants. These consist of the joint surface or epiphysis, the metaphysis and the diaphysis. The methods by which fixation in each zone can be obtained are discussed. The authors suggest that solid fixation should be obtained in at least two of the three zones and emphasise the importance of pre-operative planning and implant selection.
Keywords: Multi-zone strategy; Revision total knee replacement; Zonal fixation.
©2015 The British Editorial Society of Bone & Joint Surgery.
Learn more about the zonal fixation here
METAPHYSEAL CONES AND SLEEVES IN REVISION TOTAL KNEE ARTHROPLASTY: TWO SIDES OF THE SAME COIN?
Complications, clinical and radiological results—a systematic review of the literature A. Zanirato1 · M. Formica1 · L. Cavagnaro2 ·
S. Divano1 · G. Burastero2 · L. Felli1 Received: 10 December 2018 / Accepted: 8 February 2019 © Istituto Ortopedico Rizzoli
2019
Abstract
Revision total knee arthroplasty (rTKA) is increasing of relevance in orthopaedic surgeon daily practice and this trend is likely to continue in the years ahead. The aim of this systematic review of English literature is to summarize and compare indications, complications, clinical and radiological results of metaphyseal cones and sleeves in management of bone loss in rTKA. Retrospective or prospective studies with at least 1 year of follow-up (FU) were included. The PRISMA 2009 flowchart and checklist were considered to edit the review. Clinical and radiological results, rates of intraoperative fractures, aseptic loosening, periprosthetic joint infection, septic failure, reoperations and re-revisions were extrapolated by the papers. Thirty-seven articles were included in the systematic review. Results of 927 cones (mean FU of 3.6 ± 1.4 years) and 1801 sleeves (mean FU of 4.5 ± 1.6 years) were analysed. The studies showed good clinical and functional outcomes. Cones and sleeves allowed a stable metaphyseal fixation. The aseptic survivorship of the implants was 97.3% in cones group and 97.8% in sleeves group. Metaphyseal cones and sleeves represent a viable option in management f type IIb and III AORI bone defects in aseptic and septic TKAr with overlapping survival rate. Further high-quality long-term studies would better clarify complications, clinical and radiological results of these promising techniques in revision total knee arthroplasty.
Learn more here




Waldemar Link GmbH & Co. KG
Joint Prostheses "Made in Germany"
Products
Company
Your contact to us
69 King Street
Dover, NJ 07801
USA
Phone +1 973 625 1333
info@linkbio.com
Standard Terms & Conditions (buying, selling) | Legal notice | Conditions of use | Privacy Policy | Privacy statement for job applicants | Fernwartung
2025 © Waldemar Link GmbH & Co. KG