BiMobile Dual Mobility System

Reliable - Safe - Solution
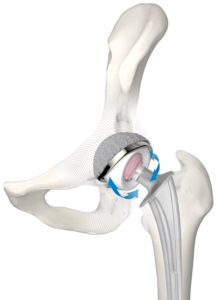
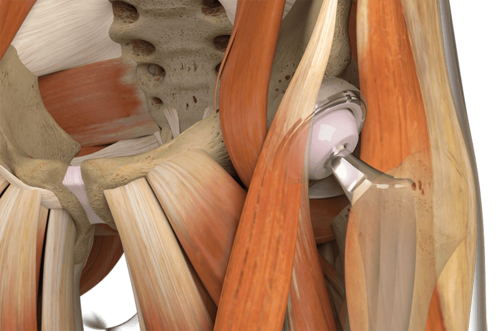
The concept of double mobility was developed by Prof. Gilles Bousquet in 1975 with the aim of treating habitual hip luxation.13 The system consists of a metal casing with a highly polished internal surface and a movable polyethylene inlay, in which a press-fitted prosthesis head moves. This provides a greater range of motion with less abrasion14, 15, 16 and reduced risk of luxation.15, 17, 18 It was on the basis of this principle that the BiMobile Acetabular Cup System came about.
The development of the bimobile acetabular cup system drew on many years of experience with successful implant systems and fixation concepts plus state-of-the-art material and coating technologies. The result is the versatile BiMobile Acetabular Cup System.
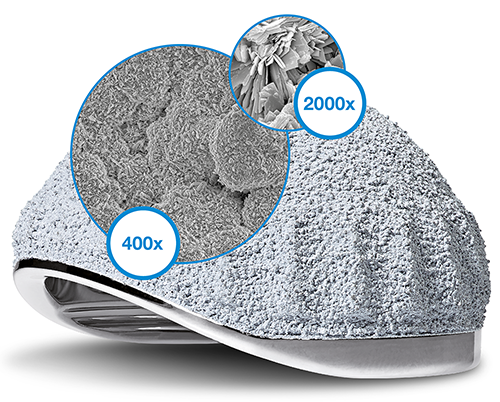
The cementless BiMobile Acetabular Cup is available with a TiCaP double coating. The TiCaP double coating combines the properties of a highly porous layer of pure titanium for primary fixation and calcium phosphate coating, which together provide optimal primary and secondary implant stability.4, 5 A special macrostructure on the cup equator increases primary stability.9
Highly wear-resistant acetabular cup1, 2, 6
The BiMobile Dual Mobility System is available in two versions, either cemented or cementless. The metal casings in both versions are fabricated from biocompatible, sturdy EndoDur CoCrMo material.1, 2 The inner surface is highly polished in order to minimize wear.
Use of known anchoring techniques
The cemented BiMobile Acetabular Cup has a finely matt-finished SatinLink surface, which is also a feature of the SP II stems. Latitudinal and longitudinal groove-like structures reinforce the fixation and allow air to escape when the implant is pressed into the cement bed.

Self-centering inlay11
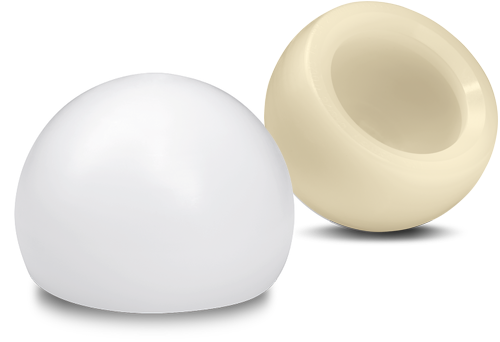
The inlays are available in UHMWPE and E-Dur (X-LINKed Vit-E PE) and can be combined with Link prosthesis heads made of CoCrMo or ceramic with a 22 or 28 mm diameter.
Features and advantages
Highly abrasion-resistant, biocompatible EndoDur CoCrMo material1, 2, 6
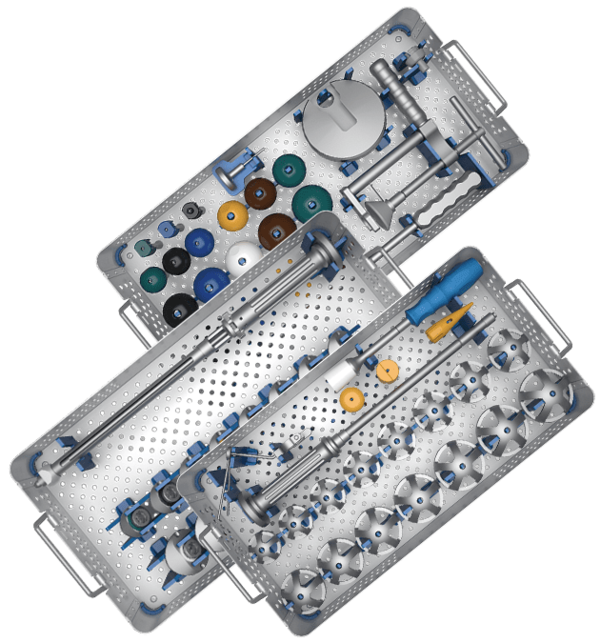
Safe implantation thanks to a fixed implant-instrument connection and unobstructed view of the acetabular cup rim11, 12
Cementless and cemented fixation
28 mm prosthesis heads starting at a cup size of 48 mm for a wide range of motion
Broad range of sizes (42–70 mm)
Clinically proven, very rough TiCaP double coating2, 3
Self-centering inlays for a uniform load distribution and increased protection against luxation7
Inlays available in Vit-E PE and UHMWPE
Anatomical medioventral recess for a wide range of motion and for protection of the femoral nerve and iliopsoas
Size-adapted clearance between liner and metal casing for constant articulation11
Intraoperative flexibility11, 12

- Internal document W. LINK (DOC-08614)
- Internal document W. LINK (DOC-08725)
- Ullmark G et al.: "Analysis of bone formation on porous and calcium phosphate-coated acetabular cups: a randomised clinical [18F] fluoride PET study." Hip International 22.2 (2012).
- Cunningham B W et al.: “General Principles of Total Disc Replacement Arthroplasty”, Spine, Vol. 28, No. 20 Suppl., 2003
- Bobyn, J. D., et al. „The optimum pore size for the fixation of porous-surfaced metal implants by the ingrowth of bone.“ Clinical orthopaedics and related research 150 (1980): 263-270.
- Long, M., & Rack, H. (1998). Titanium alloys in total joint replacement—a materials science perspective. Biomaterials, 19(18), 1621-1639.
- Fabry C, Kaehler M, Hermann S, Woernle C, Bader R. 2014. Dynamic behavior of tripolar hip endoprostheses under physiological conditions and their effect on stability. Medical Engineering & Physics 36:65- 71.
- Internal document W. LINK (DOC-08553)
- Internal document W. LINK (DOC-08695)
- Loving L, Herrera L, Banerjee S, Heffernan C, Nevelos J, Markel DC, Mont MA. 2015. Dual mobility bearings withstand loading from steeper cup-inclinations without substantial wear. J Orthop Res. 33(3):398-404.
- Internal document W. LINK (DOC-08847)
- Internal document W. LINK (DOC-07974)
- Noyer, D., Canton, J. H. (2016). Once upon a time… Dual mobility: hi story. International Orthopaedics Vol. 41 - No. 3 (March 2017): 611-618
- Charnley, John. „The long-term results of low-friction arthroplasty of the hip performed as a primary intervention.“ Bone & Joint Journal 54.1 (1972): 61-76.
- Philippot, R., Camilleri, J. P., Boyer, B., et al. (2009). The use of a dual-articulation acetabular cup system to prevent dislocation after primary total hip arthroplasty : analysis of 384 cases at a mean follow-up of 15 years . SICOT 33: 927-932.
- Wroblewski, B., Siney, P., Flemin, P. (2009). The principle of low frictional torque in the Charnley total hip replacement. JBJS (Br) Vol. 91-B(7): 855-858.
- Stroh, D. Alex, et al. "Dual-mobility bearings: a review of the literature." Expert review of medical devices 9.1 (2012): 23-31.
- Nevelos, J., Bhimji, S., Macintyre, J., et al. (2010). Acetabular Bearing Design Has a Greater Influence on Jump Distance than Head Size. 56th Annual ORS Meeting: Poster #2028.
LCU
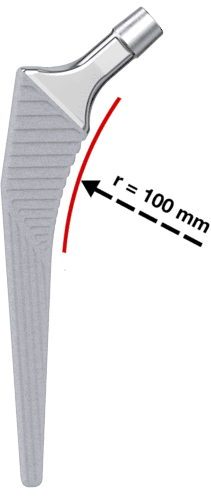
The LCU Hip System follows the concept of a straight stem with tapered lateral shoulder. The profile is straight with a rectangular cross-section.

Two offset types allow for adaption to the patient’s anatomy 2:
- Standard type with a CCD angle of 130º
- Lateralizing type with a CCD angle of 125º
The stability of the implant is additionally enhanced by the characteristic metaphyseal V-shape, while the rectangular cross-section neutralizes torsional forces. 5, 8
- Meta-diaphyseal support and fixation provided by a large medial curvature with a 100 mm radius for anatomical adaptation is the prerequisite for primary and secondary stability.
The flat, tapered prosthesis neck allows a large range of motion between prosthesis stem and acetabular cup.2
The 12/14 taper is designed for the use of modular LINK prosthesis heads made of ceramic or metal with various lengths and diameters.
Furthermore, the highly polished neck region reduces abrasion in the event of unintentional contact with the acetabular cup.9
- The stem is made from Tilastan-S (Ti6Al4V).
- The micro-roughness of the metal surface is created by corundum-blasting. This produces a regular and uniform surface structure with sufficient roughness for bone integration.2, 3
- The HX coating, a calcium phosphate layer (about 15 µm thick), is applied over the whole length of the prosthesis stem.
- The horizontal ribs in the proximal section of the stem serve to counteract subsidence of the stem and to promote primary stability. The distal region has vertical ribs to counteract the rotational forces.7



- General information on Corail-type femoral stems: Hallan, G., et al. "Medium-and long-term performance of 11 516 uncemented primary femoral stems from the Norwegian arthroplasty register." Bone & Joint Journal 89.12 (2007): 1574-1580."
- Internal documentation W. LINK
- Garcia-Rey E, Garcia-Cimbrelo E. Grit-Blasted Implant Bone Interface in Total Joint Arthroplasty. In: Karachalios T, editor. Bone-Implant Interface in Orthopedic Surgery: Basic Science to Clinical Applications. London: Springer; 2014. p. 83-9.
- Yang C., Effect of calcium phosphate surface coating on bone ingrowth onto porous-surfaced titanium alloy implants in rabbit tibiae, J Oral Maxillofac Surg. 2002 Apr;60(4):422-5.
- Hwang KT, Kim YH, Kim YS, Choi IY. Total hip arthroplasty using cementless grit-blasted femoral component: a minimum 10-year follow-up study. The Journal of arthroplasty. 2012;27(8):1554-61.
- Jones DL, Westby MD, Greidanus N, Johanson NA, Krebs DE, Robins L, et al. Update on Hip and Knee Arthroplasty: Current State of Evidence. Arthritis care & research. 2005;53:772-80.
- Vidalain, Jean-Pierre. Twenty-year results of the cementless Corail stem. International orthopaedics, 2011, 35. year, No. 2, p. 189-194.
- Khanuja H, Vakil J, Goddard M, Mont M. Current Concepts Review: Cementless Femoral Fixation in Total Hip Arthroplasty. J Bone Joint Surg Am. 2011;93:500-9.
- International Orthopedics, Volume 41, Number 3, March 2017, Page 611-618
- (Scheerlinck, T., and P-P. Casteleyn. "The design features of cemented femoral hip implants." Bone & Joint Journal 88.11 (2006): 1409-1418.)
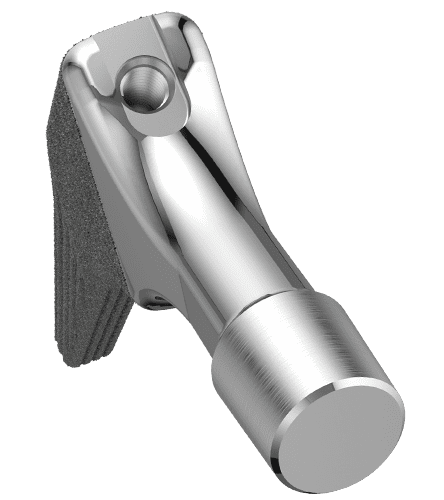
LINK Direct Anterior Approach (DAA)

ANATOMICAL APPROACH with Anatomical Stems made by LINK
Tissue preserving approach meets bone preserving stems
- Polished tip supports easy and safe insertion1
- Integrated anteversion facilitates access to the femur
- Flattened lateral shoulder helps to preserve bone and soft tissue2

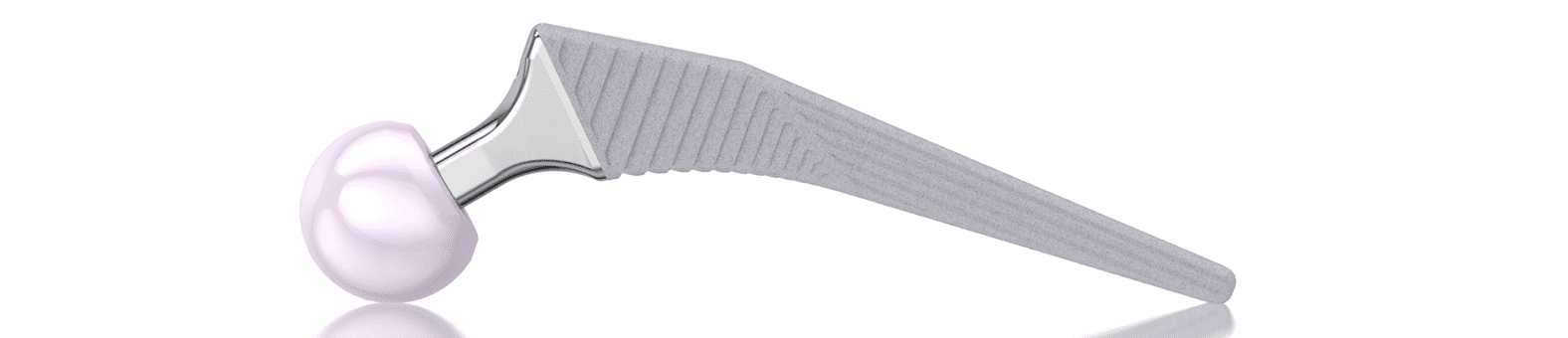
LUBINUS SPII

Neutralizes torsional forces
The curved shape of the stem enables it to finds its way into the femoral canal, where it adapts perfectly to the anatomy.6 This means that stress peaks, as occur with three-point locking of straight shafts, are avoided and the stem has greater rotational stability.2


Developed in 1978, and available with a modular prosthesis head since 1984, this femoral stem was a great success and had a major influence on the principle of the anatomical hip prosthesis.1 The S‑shaped curvature, which follows the natural anatomy of the femur, has proved highly successful in this system. This has been repeatedly confirmed over the last 40 years in numerous publications, including the Swedish Hip Arthroplasty Register.1, 3 The outstanding clinical history was the reason for developing the SP-CL, based on the same principle.
Anatomical design
The anatomical shape of the stem enables it to fit centrally in the medullary canal. This helps to ensure a uniform cement coating, which can envelop the implant optimally.7 At the same time, anteroposterior and mediolateral ribs contribute to rotational stability.2, 8, 9, 10

Optimal anatomical reconstruction
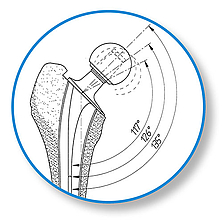
The SP II offers a system with great modularity. The multiplicity of possible variations in CCD angle, neck length, and stem length gives maximum flexibility for reconstruction of the anatomical structures in primary and revision arthroplasties. The stem tip is curved on the lateral side in order to prevent impacts when it is introduced into the medullary canal. The slender stem design meets all the requirements for minimally invasive, soft tissue, and bone-conserving implantation.
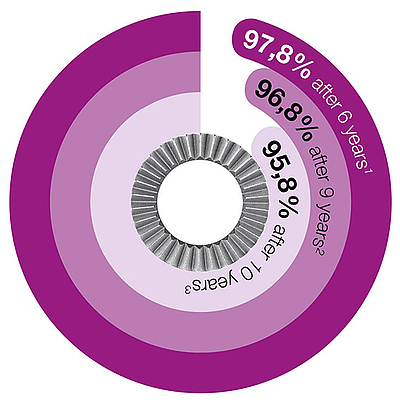
Successful long-term outcomes
Many long-term outcomes with survival rates of up to 92.3 percent after 23 years emphasize the success and great reliability of the SP II Stem.1
* www.odep.org.uk; Orthopaedic Data Evaluation Panel




- Kärrholm, Lindahl, Malchau, Mohaddes, Rogmark, Rolfson, ANNUAL REPORT 2015; The Swedish Hip Arthroplasty Register
- W.T. Stillwell. The Art of the Total Arthroplasty. Grune & Stratton, Inc. 1987; pp. 296
- H. Malchau et al; Prognosis of Total Hip Replacement, Orthopädie, Universität Göteborg, Schweden, 2002
- Malchau H, Herberts P, Ahnfelt L. Prognosis of total hip replacement in Sweden. Follow-up of 92.675 operations performed 1978-1990. Acta Orthop Scand 1993;64 (5): 497-506
- Garellick, Kärrholm, Rogmark, Rolfson, Herberts, ANNUAL REPORT 2014; The Swedish National Hip Arthroplasty Register.; p. 75
- Annaratone, Giovanni; Surace, Filippo Maria; Survival analysis of the cemented SPII stem; J Orthopaed Traumato (2000) 1:41-45. Springer Verlag
- LINK News Orthopädie aktuell, Spinger-Verlag GmbH & Co. KG, SPII® Modell Lubinus® - Stellenwert der SPII® Modell Lubinus® Hüftprothese im aktuellen Bericht des Nationalen Schwedischen Hüft-TEP-Registers von 1979 - 2002
- Langhans, M., Hofman, D., Ecke, H., & Nietert, M. (1992). Der Einfluß der Formgebung des Prothesenschaftes auf die Beanspruchung des proximalen Femurs. Unfallchirurgie, 18(5), pp. 266-273.
- Noble, P., Alexander, J., Lindahl, L., Yew, D., Granberry, W., & Tullos, H. (1988). The anatomic basis of femoral component design. Clinical Orthopaedics and Related Research(235), pp. 148-165.
- Denaro, V., & Fornasier, V. (2000). Fill, fit and conformation - an anatomical and morphometric study of a hip component in total hip arthroplasty (Rippen-Link). European Journal of Orthopaedic Surgery & Traumatology, 10(4), pp. 239-247.
- High risk of early periprosthetic fracture after primary hip arthoplasty in elderly patients using a cemented, tapered, polished stem: An observational, prospective cohort o study on 1,403 hips with 47 fractures after a mean follow-up time of 4 years· Broden C, Mukka S, Muren O, Eisler Stark A, Skoldenberg O, Acta Orthopaedica 2015; 86 (1):x-x
MobileLink


Many years of experience with successful implant systems and a range of fixation concepts, together with state-of-the-art material and coating technologies, have gone into the development of this new acetabular cup system. The result is the versatile cementless MobileLink Acetabular Cup System.
The MobileLink Acetabular Cup System comes in two different versions: A cluster-hole press-fit cup and a multi-hole press-fit cup. Both versions of the shells are available with a PlasmaLink coating or with a TiCaP double coating.
The TiCaP double coating combines a highly porous surface to achieve primary fixation and a calcium phosphate coating, which together ensure optimal primary and secondary implant stability.
The MobileLink Acetabular Cup System can be used with UHMWPE inserts. UHMWPE inserts are available in Standard UHMWPE and E-DUR (X-LINKed, Vit-E PE) versions. All UHMWPE inserts are available in a standard version and also with protection against luxation. The MobileLink Acetabular Cup System can be combined with modular offset and/or inclining casing/insert adapters (Face Changer). The adapters allow restoration of the anatomy in revision cases.

The MobileLink Acetabular Cup System can be transformed into a modular dual mobility system, with the use of Dual Mobility Inserts made from EndoDur. The DM Insert is to accommodate poly DM Liners from the BiMobile Dual Mobility System.
The dual mobility concept was developed by Prof. Gilles Bousquet in the 1970s with the aim of avoiding recurrent hip luxations. A modular Dual Mobility System is composed of a Dual Mobility Insert with a highly polished inner surface placed in a Shell in which a mobile polyethylene Liner with a pressed-in Prosthesis Head is moving.
Features and Advantages of the Dual Mobility System:
- Dual mobility leads to reduced risk of dislocation and increased range of motion (RoM) 4
- Polished inner surface for minimized wear and a prolonged implant life 5,6
- Self-centering Liner promotes even wear patterns and enhances dislocation resistance 7

Features and advantages
Wide choice of sizes (Ø 42-80 mm)
Choice of latest materials, such as E-DUR Polyethylene
Clinically proven rough TiCaP double coating2
Secure – triple fixated inserts
Unique technology of the Face Changer fixation1,3
50/36 mm – small outside, large inside
Color coding for efficient work flow
High flexibility, minimal stock holding
Intraoperative flexibility
Simple instrument set and color coding for efficient surgical procedures
Casing/insert adapter (Face Changer) for anatomical reconstruction1
Variable options for placing bone screws 1


- Data on File, Waldemar Link.
- Ullmark G, Sorensen J, Nilsson O. Analysis of bone formation on porous and calcium phosphate-coated acetabular cups: a randomised clinical [18F]fluoride PET study. Hip international: the journal of clinical and experimental research on hip pathology and therapy. 2012;22(2):172-8.
- PCT-Patent Application WO 2017/140497 A1
- Stroh, D. Alex, et al. "Dual-mobility bearings: a review of the literature." Expert review of medical devices 9.1 (2012): 23-31.
- Long, M., & Rack, H. (1998). Titanium alloys in total joint replacement—a materials science perspective. Biomaterials, 19(18), 1621-1639
- Loving L, Herrera L, Banerjee S, Heffernan C, Nevelos J, Markel DC, Mont MA. 2015. Dual mobility beari ngs withstand loading from steeper cup-inclinations without substantial wear. J Orthop Res. 33(3):398-404.
- Fabry C, Kaehler M, Hermann S, Woernle C, Bader R. 2014. Dynamic behavior of tripolar hip endoprostheses under physiological conditions and their effect on stability. Medical Engineering & Physics 36:65– 71.
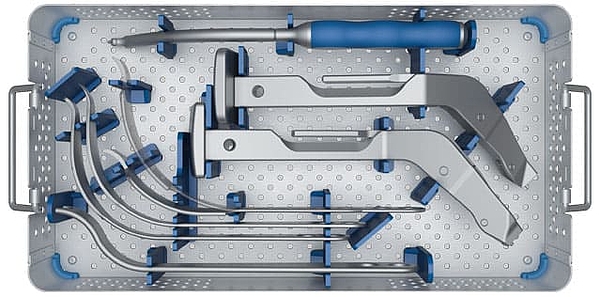
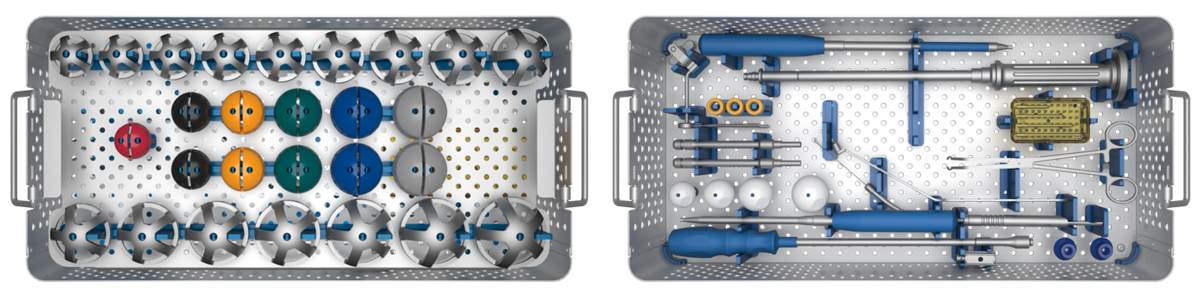
MP Reconstruction System

The MP Reconstruction System gives the surgeon the intraoperative flexibility and certainty1 that is essential for a successful revision procedure with pronounced bone loss. The system’s unique design has produced outstanding outcomes for decades.2, 3, 4
With just three instrument trays, the MP System enables a simple and fast surgery and a smooth process in five steps. The modular system gives the surgeon a high degree of flexibility in terms of adapting leg length, offset, and anteversion, independently of the distal cementless anchoring of the stem. This permits a quick and uncomplicated intraoperative response to the individual anatomy and defect.5
The stems in all six lengths have a 3° angulation, which facilitates following the anatomical curvature of the femur. The 2° tapered stem with peripheral longitudinal ribs gives outstanding stability in the femur, even with large proximal defects.2
The PowerLock toothed connection allows the stem length to be adjusted intraoperatively by means of spacers in 10 mm increments up to 30 mm for revision arthroplasties. The absence of a taper connection means that the stem length and also the anteversion and offset can be adjusted retrospectively without endangering the distal fixation of the stem.





- Postak PD, Greenwald AS: The Influence of Modularity on the Endurance Performance of the LINK® MP® Hip Stem. Orthopaedic Research Laboratories, Cleveland, OH, 2001
- Rodriguez, J. A., et al., et al. Reproducible fixation with tapered, fluted, modular, titanium stem in revision hip arthroplasty at 8-15 years follow-up. The Journal of Arthroplasty. 2014, 29.;
- Kwong LM, Miller JA, Lubinus P: A Modular Distal Fixation Option for Proximal Bone Loss in Revision Total Hip Arthroplasty. J Arthroplasty Vol. 18 No. 3 Suppl. 1 2003
- Klauser et al. - Medium-term Follow-Up of a Modular Tapered Noncemented Titanium Stem in Revision Total Hip Arthroplasty, The Journal of Arthroplasty Vol 28 No. 1, 2013, 84-89)
- Internal documents (Complaint Reports and Competitors Comparison)
MP Monoblock

Going back to the proven design features of the MP Reconstruction System, the MP Monoblock is designed to meet the needs of modern revision surgery and is completing the MP Family with a new versatility. The MP 2° taper angle and the proven, broad spline geometry give the stem a superior axial stability and lower the risk of subsidence.1 The rough, grit blasted surface of the stem made from biocompatible Tilastan-S shall support the osseointegration and bone remodelling to provide long-term stability.2 Low risk of subsidence combined with a high offset version shall minimize the risk of luxation, while the short taper and flattened neck provide a great range of motion.1, 2, 3
The surgical technique and instrumentation provides wide intraoperative versatility. The result is a system that allows the surgeon unlimited flexibility within the MP family.4
The instruments are designed to create a precise, reproducible relationship between the reamer, trial and implant positioning to help predict the ideal centre of rotation and support long-term stability of the hip joint.4

Guided insertion
fixed instrument connection
for full rotational control

Suture holes
Ø 3mm suture holes
with smooth, polished edges

Rounded tip
The tips of the stems are rounded

Neck portion
2 offset options & CCD angles
A/P flattened & polished neck
short 12/14 taper
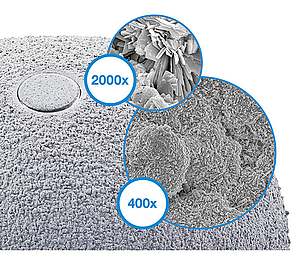
Surface
PoroLink, rough, grit blasted
surface, 200x

Distal stem portion
2° taper in the distal portion
8 to 10 ribs with broad,
tapered geometry



- Pierson J, Small S, Rodriguez J, Kang M, Glassman A. The Effect of Taper Angle and Spline Geometry on the Initial Stability of Tapered, Splined Modular Titanium Stems. J Arthroplasty. 2015 Jul;30(7):1254-9
- Rodriguez et al. – Reproducible fixation with a tapered, fluted, modular, titanium stem in revision hip arthroplasy at 8-15 years follow-up, The Journal of Arthroplasty 29 Suppl. 2 (2014) 214-218 Berry – Treatment of Vancover B3 Periprosthetic Femur Fractures with a fluted tapered stem, clinical orthopaedic and related research Number 417, pp 224-231
- Dr. med. Martin Ellenrieder. Einfluss der Defektgröße des femoralen Knochenlagers auf die Primärstabilität modularer Revisionshüftstiele - eine biomechanische Analyse (Seite 16)
- Internal Document W. Link (DOC-10571)
Waldemar Link GmbH & Co. KG
Joint Prostheses "Made in Germany"
Products
Company
Your contact to us
69 King Street
Dover, NJ 07801
USA
Phone +1 973 625 1333
info@linkbio.com
Standard Terms & Conditions (buying, selling) | Legal notice | Conditions of use | Privacy Policy | Privacy statement for job applicants | Fernwartung
2025 © Waldemar Link GmbH & Co. KG